Trichofolliculoma is a rare, benign skin tumour arising from a hair follicle containing a large central cystic hair follicle with branching epithelial strands and buds.1–5 Trichofolliculomas typically affect the head and neck, appear flesh-coloured, dome-shaped, and may also have a tuft of hair emanating from a central pit.1–5 We report a case of a 15-year-old male with a lesion of the palpebral conjunctiva with clinical and histopathologic features consistent with trichofolliculoma.
Case presentation
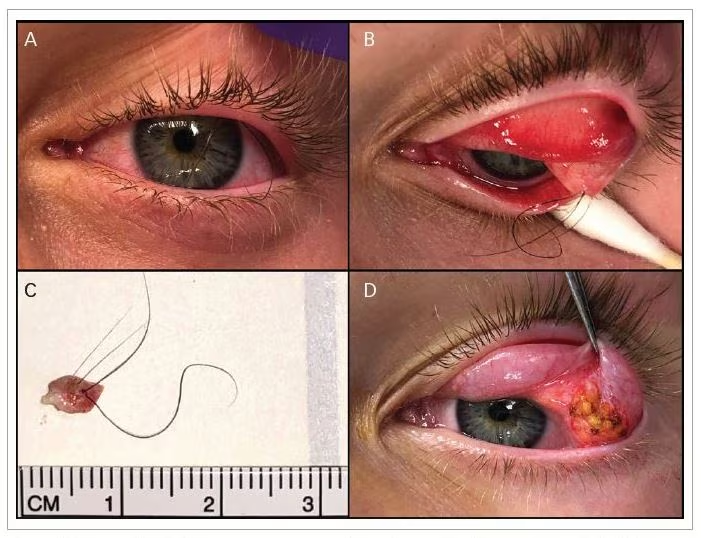
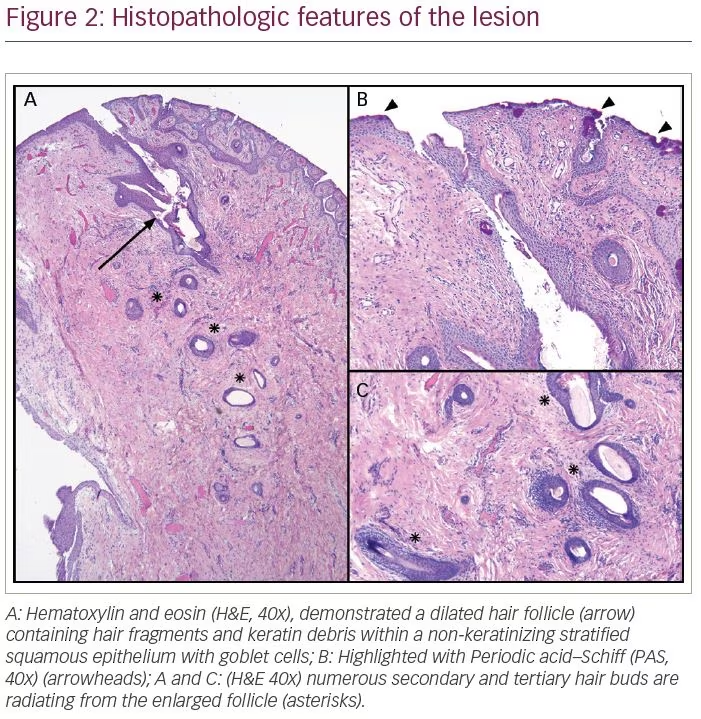
A healthy 15-year-old boy with several years of intermittent foreign-body sensation in the left eye presented with worsening eye irritation. A slit lamp examination revealed several long dark hairs emanating from the superior fornix and traversing the surface of the cornea (Figure 1A). Double eversion of the left upper eyelid with gentle pressure on the globe revealed that these hairs were originating from an elevated pink nodule of the palpebral conjunctiva in the superolateral fornix (Figure 1B). In an attempt to relieve the irritation, several hairs were removed at the slit lamp. However, the procedure was tolerated poorly, and the patient subsequently underwent complete surgical excision of the lesion under sedation. The nodule was found to be adherent to, but separate, from the lacrimal gland (Figure 1C and D). Histologic analysis demonstrated a dilated hair follicle containing several hair fragments surrounded by numerous secondary and tertiary hair follicles, consistent with trichofolliculoma (Figure 2). The postoperative course was uncomplicated, with complete resolution of the foreign body sensation.

Discussion and conclusion
Trichofolliculoma is an uncommon, benign cutaneous neoplasm with hair follicle differentiation, which typically affects the head and neck.1–5 These hamartomas can affect men and women of all ages, and represent 1.3% of all eyelid adnexal tumors.1,2 Clinically, trichofolliculomas are small, smooth, pearly nodules, and often contain a central pore with wisps of immature hair.1–5 This case shared all of these features; however, this patient’s lesion was unique due to its location in the superolateral conjunctival fornix adjacent to the lacrimal gland. Trichofolliculomas are typically seen cutaneously, given their hair follicle origin, so it is unusual to observe the lesion on a mucous membrane. Although trichofolliculoma is well known to originate on the skin of the eyelids,5 this is the first reported case of trichofolliculoma arising from the palpebral conjunctiva reported in the literature.
The characteristic histologic findings of a trichofolliculoma include a dilated follicle within the upper dermis containing keratin debris and hair shafts.1–5 In addition, numerous smaller hair follicles radiate from the primary central pore.1–5 These features are evident in this case (Figure 2). However, there is also non-keratinizing stratified squamous epithelium with goblet cells, highlighted by Periodic acid–Schiff stain (Figure 2B), consistent with the trichofolliculoma arising from the palpebral conjunctiva. Given the presence of a central pore and cystic space continuous with the surface, the differential diagnosis also included dilated pore of Winer and pilar sheath acanthoma.4,6 However, this lesion lacks elongated rete ridges or lobules of infundibular cells extending from the enlarged follicle, which are seen in dilated pore of Winer and pilar sheath acanthoma, respectively.4,6,7. Dermoid cyst was also considered due to the lesion’s location in the superolateral fornix, though the absence of other adnexal structures, such as sebaceous glands, contiguous with the lesion made this diagnosis less likely.
The treatment of choice for a trichofolliculoma is complete surgical excision.1,8 Despite being a benign tumour, incomplete excision of a trichofolliculoma has been associated with recurrence.1,5,8 Also, merely epilating the lesion can cause an inflammatory reaction and subsequent scar tissue formation.1 Fortunately, this patient achieved a successful postoperative outcome with no injury to the lacrimal gland.