




The use of anti-vascular endothelial growth factor (anti-VEGF) agents has revolutionised the treatment of exudative age-related macular degeneration (wet AMD). Multiple clinical studies have shown that beneficial functional and morphological responses can be obtained with either fixed dosing or as-needed (pro re nata [prn]) treatment regimens.1–4 The treat-and-extend regimen (TER) is also used by a significant number of treating specialists with similar results, although it has not been investigated in a major multi-centre trial.5 However, stratification of patients in the Comparison of AMD Treatment Trial (CATT) study by visual response over both 1 and 2 years shows that between 12 % and 20 % of patients lose 5 or more letters in either the first year or over 2 years of treatment; between years 1 and 2, 28–34 % of patients lost 5 or more letters.3,6 In the PIER study, a multi-centre, randomised, sham-controlled trial, 34 % of patients had no initial gain from anti-VEGF and lost over 5 letters at 1 year, and an additional 40 % of patients lost their initial vision gains at 1 year.7 These patients may be considered to show a reduced response to anti-VEGF therapy, and therefore an alternate or adjunctive therapy would be useful in their long-term management.
Ionising radiation (IR) has been proposed as an adjunct treatment for wet AMD due to its complementary mechanisms of action, both structural via arresting division in a high percentage of irradiated retinal endothelial cells even by a single dose of 5 Gy, and by functional effects via decreasing vascular permeability and increasing blood flow velocity.8 Anti-angiogenic therapy is primarily anti-exudative and not anti-neovascular, hence the neovascular AMD lesion persists causing visual degradation over time. IR is anti-neovascular, causing apoptosis of the neovascular endothelium by damaging cellular DNA. IR is also known to cause pericyte knockdown in maturing vessels,9 re-exposing VEGF receptors and potentially enhancing choroidal neovascularisation (CNV) lesion regression through anti-VEGF-induced disruption. Additionally, IR can cause microfibroblast apoptosis and the reduction in cellularity of inflammatory infiltrate, reducing fibrosis
formation and inflammatory response.10–12 IR in combination with either anti-VEGF or anti-platelet-derived growth factor (PDGF), or both, results in enhanced endothelial apoptosis and reduced endothelial cell migration compared with either agent alone.13 Besides, IR is able to reduce the macrophage-mediated retinal inflammation and causes a capillary closure, both reducing a local oedema of the retina.8 Since IR effects are dependent on cell division cycles, the timeframe for observing an effect will vary by patient, normally between 3 and 9 months post-treatment. It is therefore important to have an anti-VEGF load in the vitreous at the time of stereotactic radiotherapy (SRT). Nevertheless, these biological and anatomical effects of IR clearly depend on fraction size and fractionation schedules, with higher single doses being less dependent on cell cycles and proliferation rates of cells. This is important especially for modern highprecision radiation therapies, aiming to irradiate by brachytherapy14 or with non-invasive stereotactic techniques in single fractions, by using either protons or conventional photons.8
SRT using micro-collimated 100 kilovolt X-ray has been shown in the INTREPID study to preserve vision while simultaneously sparing anti-VEGF injections. The study design and results have been previously reported.15 The study examined the effect of SRT adjunctive to anti-VEGF therapy versus sham SRT and anti-VEGF mono-therapy in patients diagnosed with wet AMD within 3 years of enrolment who had received a minimum of three injections in the previous year and who required additional anti-VEGF therapy due to new or recurring oedema or leakage. At 1 year, patients in the active SRT arm required 33 % fewer injections to maintain non-inferior vision results. Eyes with lesions whose greatest linear dimension fit within the X-ray beam spot on the retina, and with significant oedema (macular volume ≥95 % of normal on optical coherence tomography [OCT]) required 55 % fewer injections, and maintained over 5 letters of superior vision at year 1.16 The beneficial effect was maintained through year 2, although slightly reduced.17
Recently, an intraocular β-radiation delivery system was developed to treat wet AMD using an epimacular brachytherapy (EMBT) technique. A probe containing a beta-emitting strontium 90/yttrium 90 (Sr90/ Y90) source is placed over the CNV lesion in a vitrectomised eye and held in place for 3 to 4 minutes to deliver a 24 Gy dose. The technique was studied in two large multi-centre studies. Published 2-year efficacy data from the Epimacular brachytherapy for neovascular age-related macular degeneration (CABERNET) study did not support use of the technique, failing to show non-inferiority in vision compared with anti-VEGF monotherapy.14 There are important differences between SRT and EMBT that could lead to differences in clinical results. First, the β-radiation source used in EMBT delivers a point dose immediately adjacent to the source, with dose decreasing very steeply with distance, and is therefore dependent on precise and controlled placement by the retinal surgeon directly above the area of greatest CNV lesion activity during the 3 to 4 minute dose deposition. Second, because the eye is vitrectomised, the half-life of anti-VEGF in the eye is reduced.18 This has the potential effect of reducing the VEGF binding capacity, and any anti-VEGF load at time of EMBT or during subsequent PRN treatments is therefore less effective in stabilising the disease. None of these are inherent issues in SRT, since the X-ray depth dose decay is minimal within the thickness of the retina, the X-ray beam is robotically positioned and tracked throughout the treatment, and the therapy is non-invasive, leaving the vitreous intact.
Opinion
Clinical management of wet AMD is compounded in difficulty with the acceleration of new cases with the wave of the Baby Boom finally upon us, the long history of smoking and exposure to intensive light in modern western lifestyles, coupled with the maintenance of the existing chronic patient population. At our clinic in Binningen (Basel), Switzerland, wet AMD patient numbers are increasing, and many patients have been undergoing anti-VEGF treatment for many years. A significant number of these patients have exhibited persistent disease activity since first presentation, or have had disease activity recur and now persist. For patients with the need for high-frequency (4- or 6-weekly) treatment, the aim is to lighten the burden of treatment in these patients as well as to reduce the socio-economic costs. In the past, to achieve this, combinations of anti-VEGF with Verteporfin PhotoDynamic Therapy and radiation therapy were used.19,20 Failure to eliminate persistent oedema and leakage indicates poor long-term outcomes, and for these patients an alternative is necessary.
Our patients with chronic, persistent or very frequently recurring disease activity correlate well to the patients enrolled in the INTREPID study. Responder analysis indicates that choroidal neovascularisation (CNV) lesion size ≤4 mm in greatest linear diameter (GLD), abnormal macular volume and limited fibrosis are positive response predictors.16 A closer look at the data also shows that time since diagnosis or number of previous injections are not correlated with outcomes, leading to the conclusion that morphological parameters should be used exclusively to determine if a patient is a good candidate for SRT.
Practical Application
As an early first adopter of this technology (our first patient was treated in August 2013), we tended at first to screen patients who had the greatest chronic need: those that had been under therapy for a considerable number of months or years, with nearly monthly injections. Our treatment regime is TER, and the initial patients screened for SRT consistently presented with macular fluid and therefore could not be extended beyond 4- or 6-week intervals, and in selected cases (i.e. those with high treatment burden) 8-week intervals. Our screening process was triggered by a patient need for an injection. Records were then screened for indication of reduced response to anti-VEGF monotherapy. The patient’s lesion size, macular fluid load and amount of fibrosis were evaluated. Patient selection criteria included:
- Persistent CNV-activity despite 4-weekly anti-VEGF-injections or
necessity for frequent injection treatments in the course (4- or 6
weekly; in case of high burden to the patient with 8-weekly injections
these cases might apply as well). - Substantially all lesions within the central 4 mm circle (beam diameter).
- No advanced fibrosis of the lesion.
- No advanced retinal pigment epithelium (RPE)-atrophy zones.
- Axial length <26 mm.
If these criteria were met, the patient was recommended for SRT, including a briefing by the radiotherapist and the medical physicist on IR mechanisms of action and radiation safety. With consent, the patient was scheduled for SRT within 2 weeks of their injection, following the INTREPID protocol.
SRT is performed using the IRay® Radiotherapy System (Oraya Therapeutics, Inc., Newark, CA, US). The radiation unit produces a highly collimated, narrow X-ray beam. The dose is delivered in three closely
spaced sequential applications within one session through different entry points in the inferior pars plana of the affected eye, usually applied within less than 60 minutes in total. The sequential beams converge on the retina, delivering a 16 Gy dose to an area 4 mm in diameter, centered on the fovea. The procedure starts with treatment-day machine checks (morning check of the radiation unit, machine self-test, check of the dosimetry units, standard operating procedure [SOP] checklist completion). The patient is consented including patient education of the procedure, and then patient dependent dosimetry is determined by measuring axial length. The patient is prepared with topical eye numbing drops, the head is positioned for proper alignment with the robotic X-ray delivery system, the I-Guide Eye Stabilisation unit is placed (this also serves as the stereotactic frame of reference for the robot), the eye and robot are co-aligned, treatment planning is confirmed, SOP treatment authorisation given and then delivery of the radiotherapy is administered. The patient is then provided with after-treatment instructions. Duration of the treatment session varies, dependent on patient mobility and motor function, face and eye structure (for co-alignment and scleral clearance) and the amount of eye saccadic motion during treatment, which may cause IR termination and eye re-alignment. Normally, each treatment session in total takes 30 to 60 minutes, with the actual radiation portion lasting 5 minutes or less. The patient may be required to sit quietly with slightly bowed head for about 30 minutes, about 20 minutes in a fixed
position on the system’s chin rest.
After the treatment session the patient is given after-treatment instructions and a visual ophthalmic examination. The most common immediate effect of the therapy is a slight corneal discomfort due to the application of the I-Guide, but this typically resolves in a day, and may require wetting drops.
Illustrative Case Studies
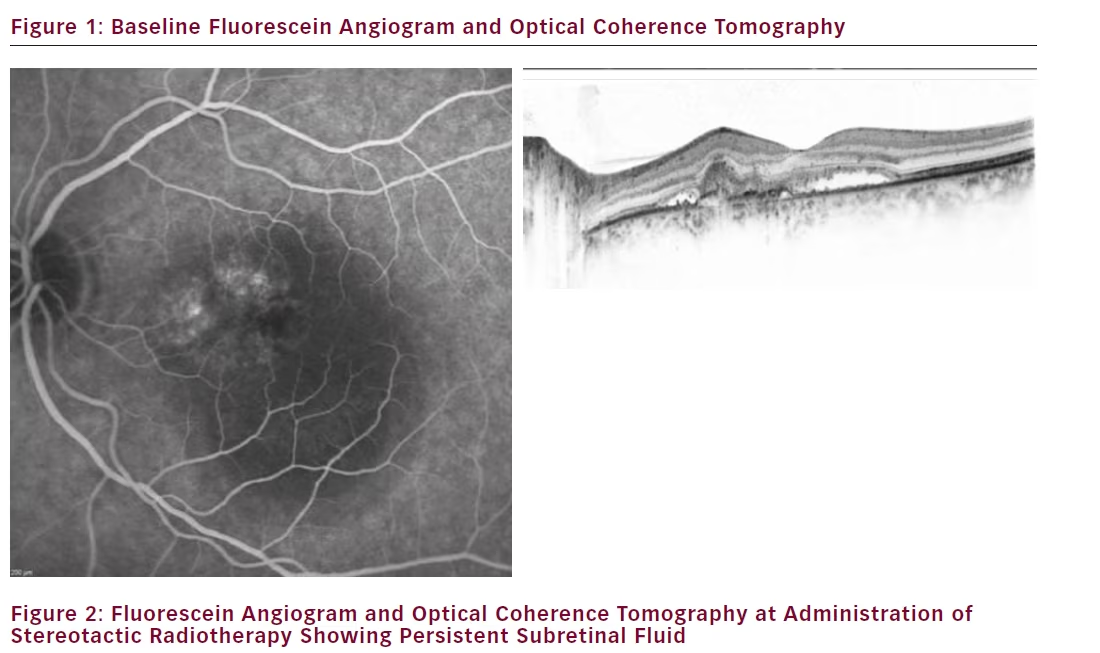
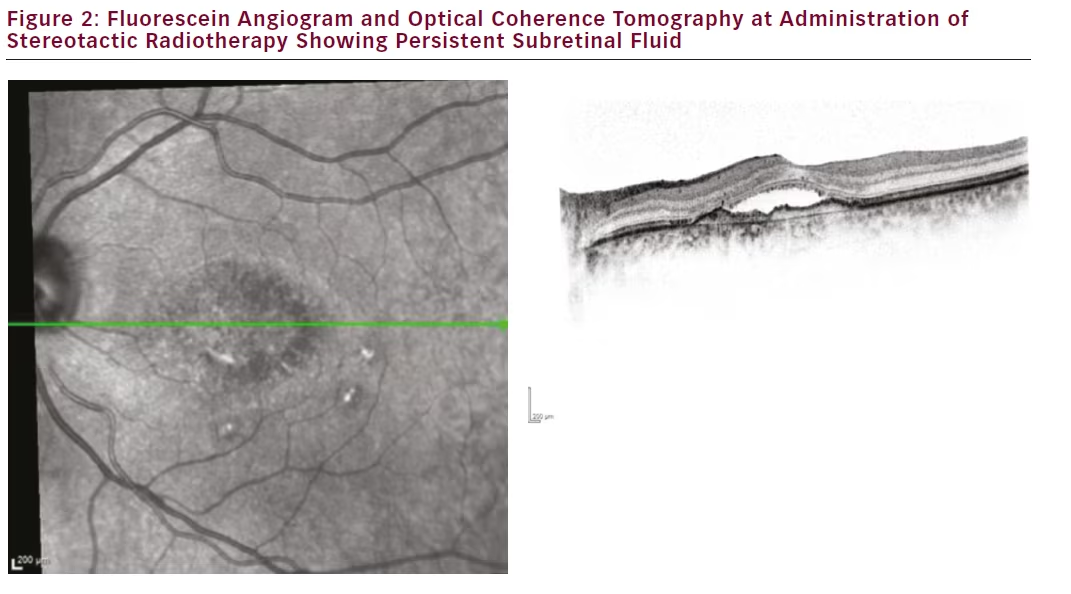
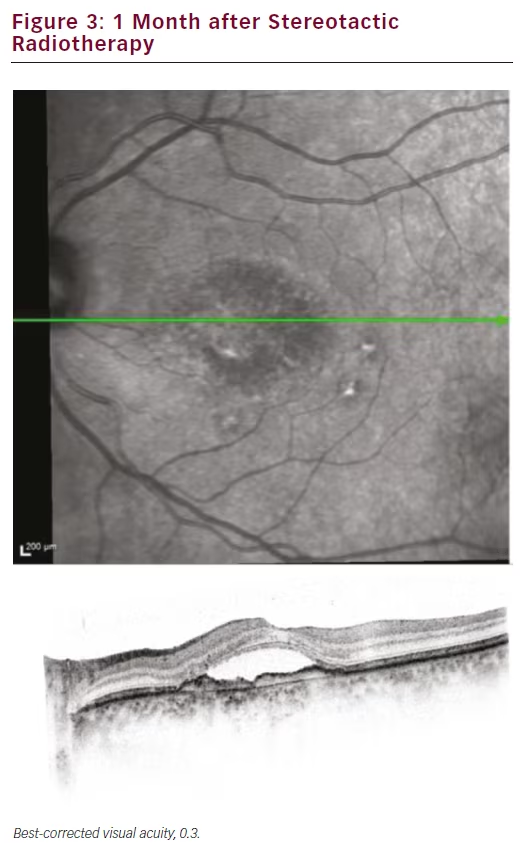
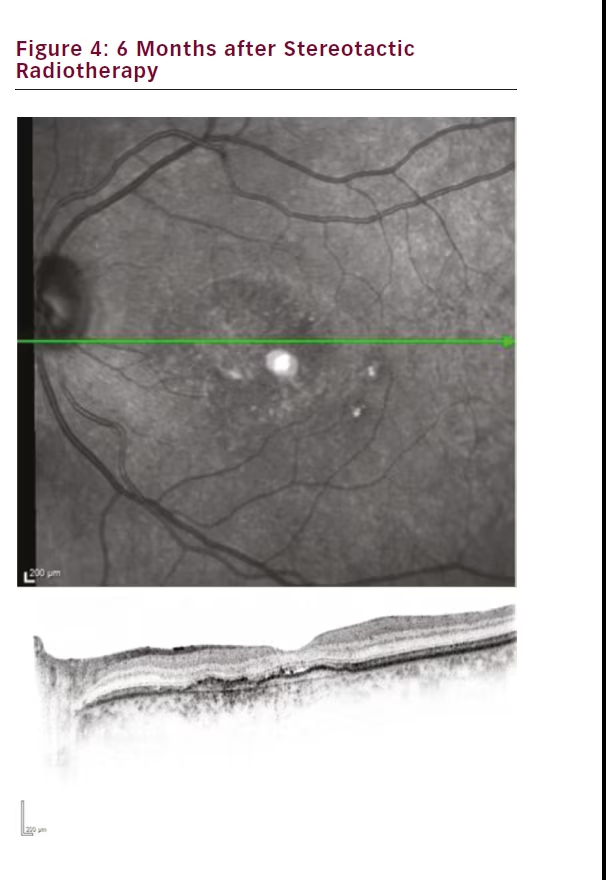
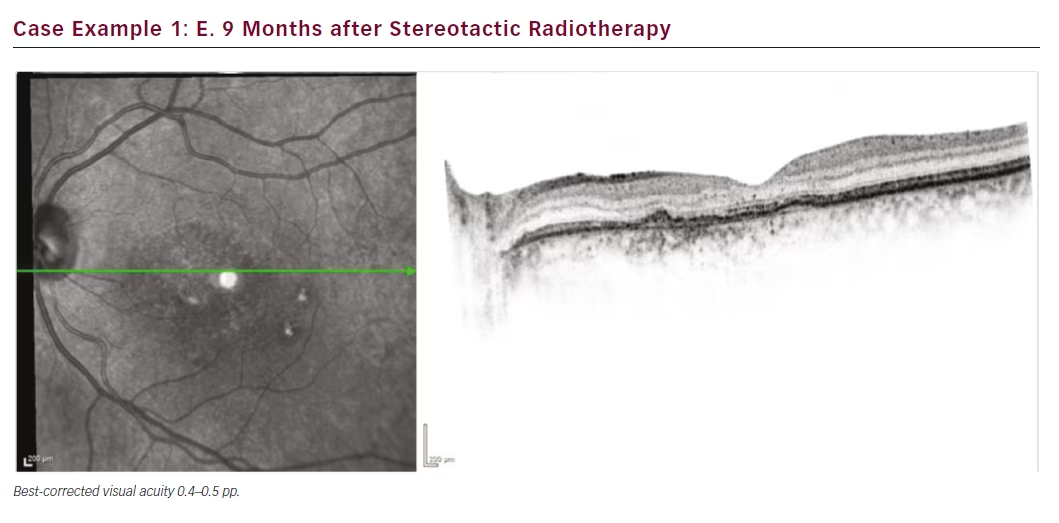
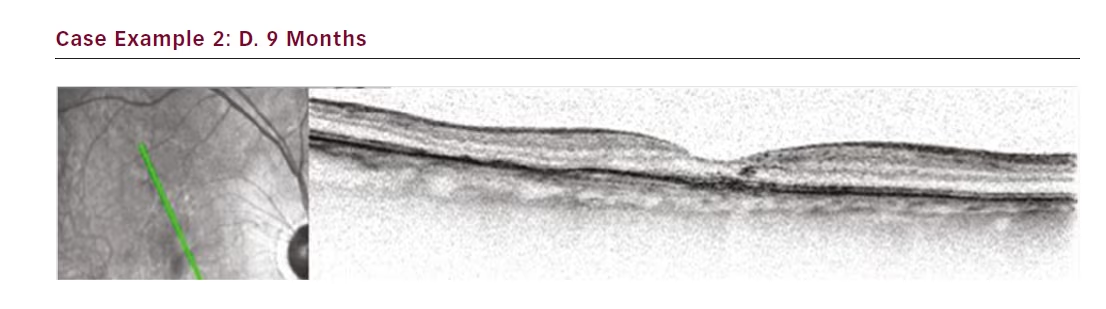
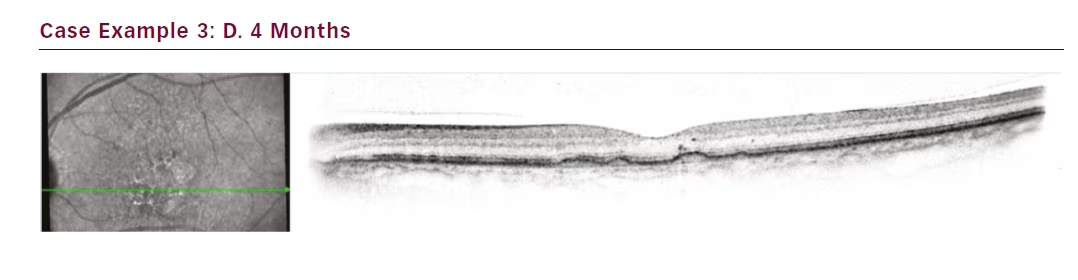
Our first treated patient was a male diagnosed with wet AMD in 2011 with a baseline best-corrected visual acuity of 0.4. He had a centrally located lesion with slight RPE detachment nasal of the foveola, and subretinal fluid (see Figure 1). In 2012, our clinic switched from a PRN to a TER regime and this patient was maintained on a 4–5 week treatment interval. Despite 21 anti-VEGF injections the eye never dried out and continued to exhibit persistent subretinal fluid and visual acuity at 0.4 (see Figure 2). The patient was also suffering from moderate to severe Sicca syndrome with an added negative effect of local anaesthetic and disinfectant drops to the dry surface after each anti-VEGF treatment. Therefore we were looking for a way to extend his treatment intervals while maintaining or improving vision. At this point SRT with the IRay system was performed, and the patient was maintained on 4-week treatment intervals. The subretinal fluid persisted without resolution for 3 months (see Figure 3), but between months 3 and 6 the subretinal fluid was nearly fully resolved (see Figure 4). The patient was maintained on 4-week intervals, and by month 9 the retina was completely dry and so the interval was extended to 6 weeks (see Figure 1E). By month 12 the retina remained dry and visual acuity improved to 0.5, so his treatment interval was further extended to 8 weeks (see Figure 1F). The OCT images show a shrinkage of the CNV lesion between 3 and 12 months.
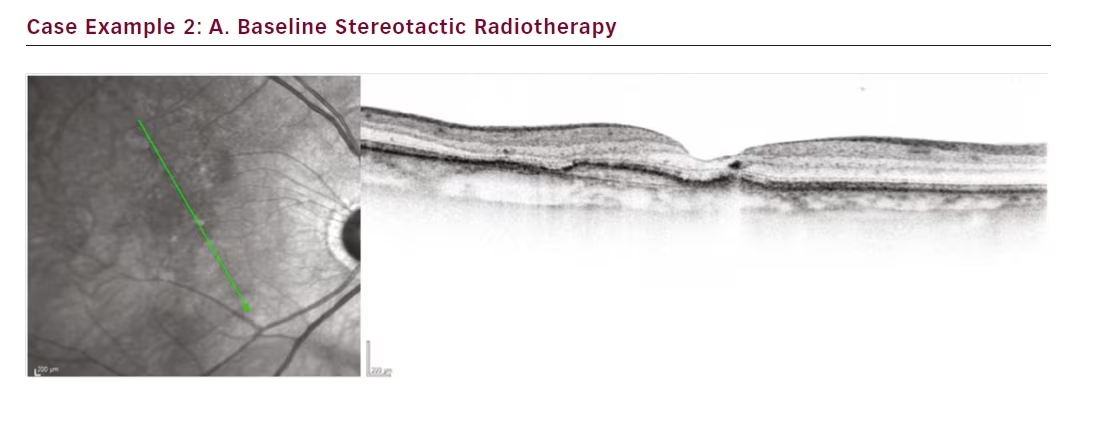
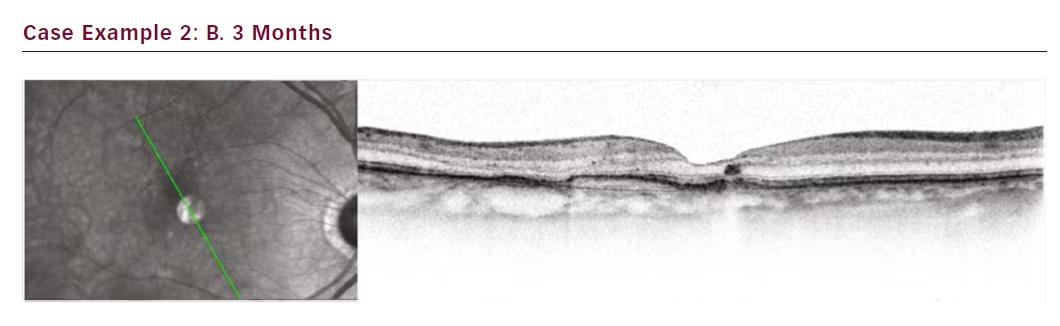
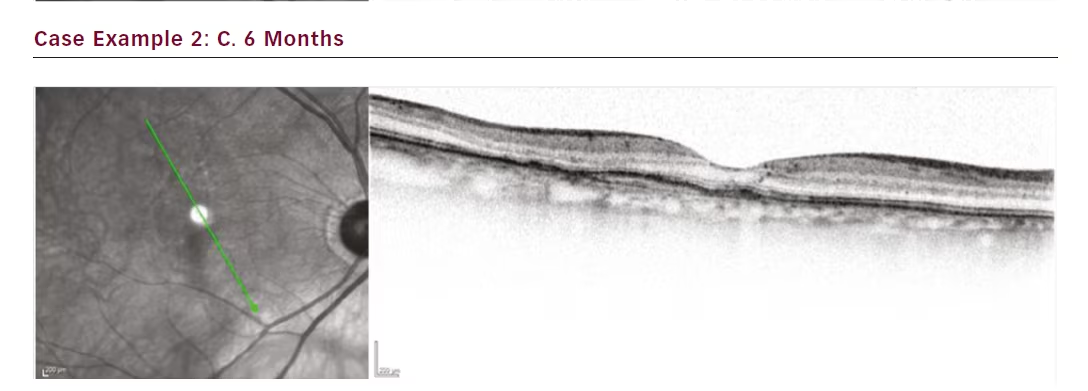
Case 2 is a female with a smaller lesion that was maintained under control with treatments at 4-week intervals, with a history of 35 anti- VEGF injections. Earlier attempts to extend the interval to 6 weeks resulted in fluid recurrence. The patient wanted a treatment option that could extend the treatment interval in order to reduce the burden of monthly follow-up visits. SRT was applied and the patient was followed at 4-week intervals through month 3 at which time we were able to start increasing the treatment interval without risking fluid recurrence. The interval was eventually increased to 12 weeks by month 9. Her visual acuity remained unchanged at 0.63 from SRT baseline. Thus we were able to meet the patient’s request successfully (see Figures 2A–D).
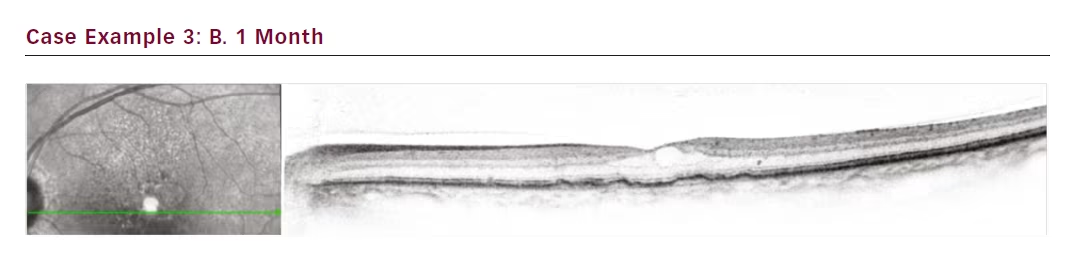
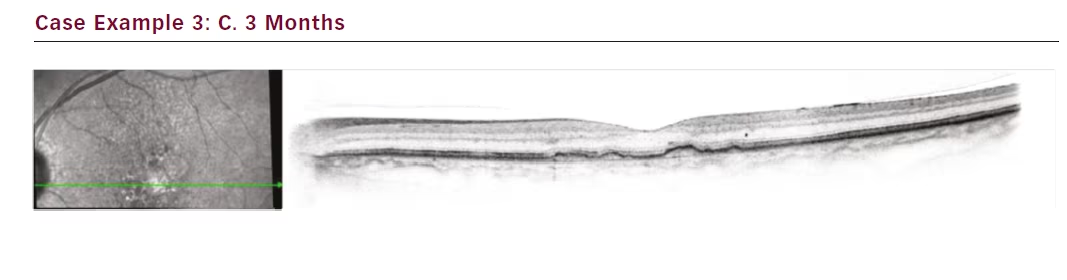
The third case is a female patient with a small lesion that remained fluid filled despite 4-week treatment intervals totalling 16 injections (see Figure 3). Attempts to extend to 6 weeks resulted in even greater

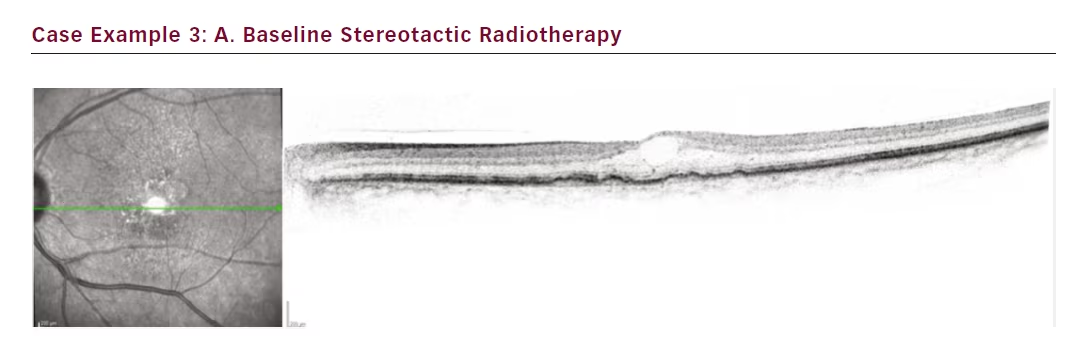
oedema. Our aim in this case was to get the lesion under control. SRT was administered and after only 1 month the lesion fluid started to resolve. At 3 months the fluid was completely resolved, and by month 4 the interval could be extended to 6 weeks. Subsequently she was moved to an 8-week interval.
Conclusion
Our experience with more than 100 treated patients has shown that SRT is a useful adjunct to anti-VEGF therapy in the resolution of persistent fluid for patients with wet AMD. Initially we treated patients who can be classified as reduced responders to anti-VEGF, characterised by chronic
fluid despite 18 to 36 months of monthly injections. Patients were selected based on the INTREPID responder analysis. The radiotherapy effect became noticeable after 3 to 9 months, consistent with the theoretical mechanisms of action and with INTREPID study results, which showed a divergence in the cumulative mean number of anti- VEGF injections between the study arms after week 12. Morphological results were impressive, with patients achieving significant reductions in central retinal thickness. Vision was maintained at levels equivalent to vision at time of SRT. This is expected given the length of time since disease onset for these patients. The treatment is well tolerated with no safety concerns noted to date. With our initial positive results we are now screening patients closer to time of diagnosis with the hope of preserving more vision before disease progression, and to define the best subgroup of patients gaining the highest profit from the effects of IR and, maybe, even fewer injections of anti-VEGF injections. Besides, safety aspects will be considered, to avoid long-term side-effects of radiation therapy by using robust fixation, precise navigation and an optimal dose decline in normal retinal tissue by the non-invasive stereotactic technique.


