




Over the last two decades, deep anterior lamellar keratoplasty (DALK) has re-emerged as a procedure
of choice, for patients with corneal stromal disease, requiring corneal transplantation. Despite
the fact that there are distinct advantages of DALK over penetrating keratoplasty (PK), the uptake
of the procedure worldwide, has been very variable. The advantages of DALK include less intraocular
complications (since it is predominantly an ‘extra-ocular’ procedure), fewer postoperative
complications, the eye being tectonically stronger than PK, less risk of allograft rejection, better
endothelial cell count postoperatively compared to PK, and less rigid requirements for the donor
cornea. For DALK, I routinely use tissue that is 10–14 days old from harvest, with low endothelial cell
count. This expands the donor pool, ‘saving the better tissue’ for endothelial keratoplasty.
Despite all the advantages of DALK over PK, the outcomes reported in the literature are very
variable. The Singapore Corneal Transplant Database tracked outcomes of DALK over 16 years, and
overwhelmingly shows better graft survival compared to PK.1 This has a profound effect on my
surgical workload, where anterior lamellar keratoplasty accounts for 30% of all my transplant cases
and is the second most common transplantation procedure I perform, behind Endothelial keraoplasty
(58%). PK being relegated, well and truly, to third place. However, data from the Australian Corneal
Graft Registry shows worse outcomes of DALK compared to PK and in the US, DALK only accounts for
2% of all transplant procedures performed (EBAA 2015 Data).2
The vast differences in outcomes and also in the percentage of cases undergoing DALK in different
centers is certainly down to the complexity of the procedure and the familiarity of how to handle
complications associated with the procedure. I would like to say that there is a learning curve to the
procedure, but I really do not think there is! A learning curve implies that once a person has gained
sufficient experience and is on the plateau at the top, cases become straightforward. However, this
appears not to be the case with DALK, and even experienced surgeons can get caught out. The
learning curve however, is in handling complications when they occur or preventing the complications
from happening. In this editorial, we will cover four tips, i.e., the ‘ABCD’, to help surgeons perform
DALK. This is not an exhaustive list but just some tips I have found useful.
A: A is for anesthesia and attitude. It is important to have the appropriate mind-set before surgery.
If you are regularly performing PK now, and want to start DALK, you have nothing to lose to try, since
at worst, the patient will get a PK, which you were going to perform anyway. For every patient with
stromal disease I routinely see in clinic who requires a corneal transplant, I will consider doing a DALK
procedure. Everything is DALK-able! It is also important to have the correct anesthesia. It is not easy
to perform a procedure on Descemet’s membrane (DM) with the patient moving. Ideally do your cases
under a general anesthesia with paralysis. It is important to ensure that there is no excessive pressure
in the anterior chamber, since this will increase the risk of rupture of the DM. Give yourself time to
perform the procedure. DALK will take longer than a routine PK.
B: B is for balance and be calm. It is important to have balance in the anterior chamber. The deeper
you go with your dissection the more you will see the DM bulging. Ideally use a non-compressive
globe speculum. I routinely use a Jaffe speculum to avoid excessive
pressure on the globe during surgery, which will raise the intraocular
pressure (IOP). It is important to decompress the anterior chamber to
reduce the IOP and prevent the bulge. This will ensure the DM is more
lax, and reduce the risk of rupture. Often, during a case, I will decompress
the anterior chamber a few times since it will reform with aqueous during
surgery. If you perforate the DM, which will definitely happen sometime in
your career, keep calm. Stop and assess the situation. The management
of a perforation will depend on the time during the procedure that it has
occurred, but in the majority of cases, the case can continue without
conversion to a PK. In cases of micro-perforation, it is always best to use
an interrupted technique when suturing, to help control the tension in the
graft. If I perforate early in the procedure, I will often suture the graft with
the anterior chamber full of air. This helps to tamponade the DM against
the stroma, but the air must be removed at the end of the case.
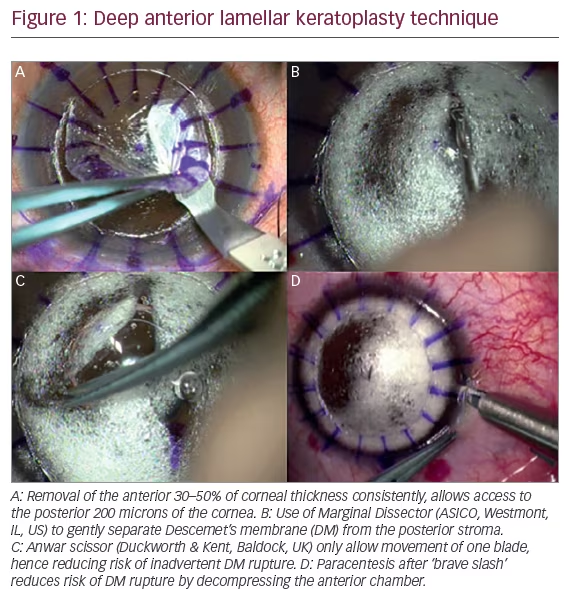
C: C is for consistency. Try to make some of the procedure consistent
regardless of which technique you will subsequently be using. I will always
remove at least 30–60% of the cornea first, before tackling the posterior
stroma. This is irrespective of whether I am performing a routine ‘big
bubble’ DALK in a patient with keratoconus, or doing a DALK in a patient
with previous hydrops, or doing a DALK in a patient with active infectious
keratitis. By repeating the first steps of the procedure multiple times, I do
not have to change my technique during more routine cases. I am also less
tense in more complex cases. Tectonic cases with full thickness perforation
are the exception to this statement, where I do alter my technique. For the
vertical lamellar depth cuts, I use a Hanna Trephine System (Moria, Antony,
France) since it has excellent accuracy on the vertical cut. However, you can
use other guarded trephines or a femtosecond laser to achieve accurate
cuts as well. It is also important to be consistent with the instruments you
use. I use the same instruments on every single case so that I am familiar
with how they work and how they feel. I prefer to use very fine forceps to grip
the stroma during dissection, normally 0.10 mm Bonn forceps (Duckworth &
Kent, Baldock, UK). They are atraumatic for the cornea and allow you to feel
the tension on the stromal tissue. For the initial dissection, I will use a sharp
2.3 mm crescent blade made by BD (Chicago, US). For the stromaectomy
around the graft edge I use the Anwar scissors (Duckworth & Kent, Baldock,
UK). For my deep lamellar dissection and DM bearing surgery, I use a
marginal dissector (ASICO, Westmont, IL, US). If I am performing ‘big bubble’
or ‘viscobubble’ I will use the Tan DALK Cannula (ASICO). You can off course
perfrom DALK using other instruments, but I have found these the most
useful in reducing intra-operative complications.
D: D is for Descemet’s membrane. A lot of people think, if they do not
‘bear’ the DM during the procedure, they have failed. This is not true. A good
deep manual technique will also give good visual acuity. However, it may take
longer to achieve that good vision. There are several techniques reported
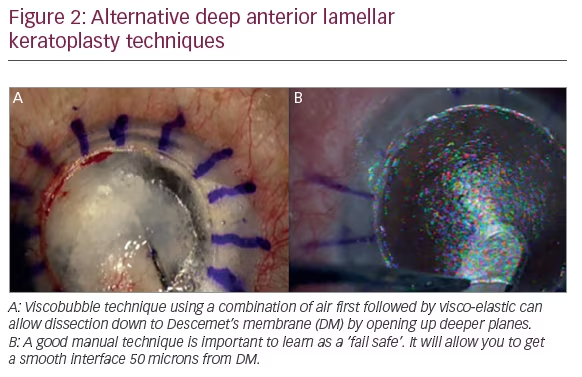
in the literature to bear the DM. These include the ‘big bubble’ technique
using forceful injection of air, visco-elastic dissection, a combination
of visco-elastic and air, manual layer-by-layer dissection, and the use of
balanced salt solution to hydrate the cornea. I will use a combination
of these techniques to achieve DM bearing DALK. It is important to be well
versed or at least familiar with all these techniques. However, in other cases
I will aim to perform a good deep manual technique – using our previously
published technique, aiming to be approximately 50 microns from the
DM. The decision on which technique to perform should be made in the
clinic not in the operating theatre. Assessing the depth of posterior scars
from multiple angles and the depth of lesions using a slit beam or anterior
segment optical coherence tomography (OCT), can be helpful. Indecision at
the time of surgery about what kind of DALK you are trying to achieve, will
lead to indecision during the surgery. If you can do a good manual DALK,
this will always be your back up plan.
The future of DALK has to be to de-skill the surgery further. Technology may
play a significant role, such as the use of femtosecond lasers or integrated
OCT. This will then hopefully increase the widespread dissemination of
this technique.


