




Ocular residual astigmatism
The initial step of planning any refractive laser treatment that requires correction of astigmatism is to calculate the difference in magnitude and axes between the refractive cylinder at the corneal plane, and the corneal astigmatism – that is the vectorial difference. This has been defined as the ocular residual astigmatism (ORA) and is expressed in dioptres (D).1 When calculating the ORA, the refractive cylinder needs to be converted to a positive magnitude at the corneal plane to allow accurate comparison to the corneal astigmatism. Several values of the ORA can be calculated for any one eye depending on which readings have been used for corneal astigmatism and which for refractive cylinder. Typically, the refractive cylinder and axis, as measured by the manifest refraction, is used for the refractive astigmatism parameter, although the cycloplegic, ocular wavefront or automated refraction can be used. The same applies for various measures of corneal astigmatism. Again, typically this is measured using a topographer, or more accurately with a tomographer, to include the posterior cornea, but one can also use automated keratometry from partial coherence interferometry devices, manual keratometry or corneal topographic astigmatism (CorT) which has been shown to be a more accurate measure of corneal astigmatism than simulated keratometry, manual keratometry and autokeratometry.2,3 The combination of refractive and corneal parameters that result in the lowest magnitude of ORA preoperatively are typically the best matched and therefore the most accurate. The average ORA lies somewhere between 0.73 D4 and 0.81 D.1 In more irregular corneas, such as keratoconus, the mean ORA has been calculated as 1.34 D,5 somewhat higher than regular corneas. An ORA of 1.00 D or greater is deemed to be significant and considered a red flag. The ORA will enable the surgeon to determine preoperatively whether all the astigmatism can be corrected or whether a residual amount will remain postoperatively on the cornea, potentially causing a suboptimal visual outcome. Subsequently, the patient can be advised on the expected outcome of refractive laser surgery. In cases where the treatment is predominantly astigmatic, for example plano/-2.00 x 75 on a near spherical cornea, and the ORA is high, then treatment by refractive parameters alone should be avoided and Vector Planning® (ASSORT Pty. Ltd., Cheltenham, Victoria, Australia)used as the preferred method as this will optimise the amount of astigmatism that can be treated and left remaining on the cornea.
Corneal topographic astigmatism
CorT is an accurate measure of corneal astigmatism based on all the measured data acquired from topography or tomography, and is calculated using the iASSORT® software (ASSORT Pty. Ltd., Cheltenham, Victoria, Australia; www.assort.com). CorT anterior is calculated using the front surface of the cornea only, based on topography, while CorT total incorporates the posterior cornea into the calculation for total corneal power using a tomographer for acquisition.2,3
Vector Planning
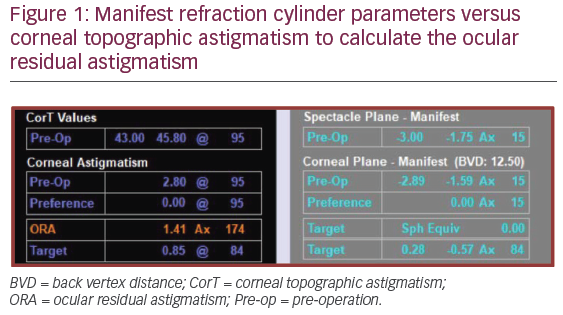
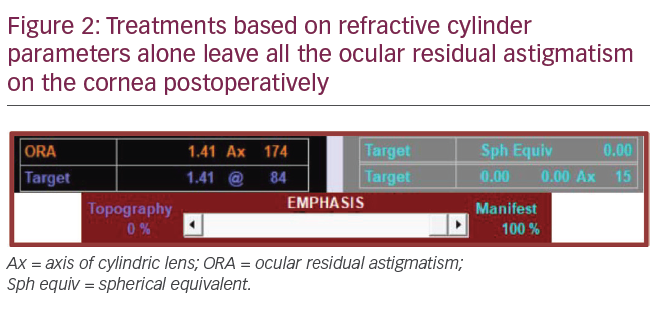
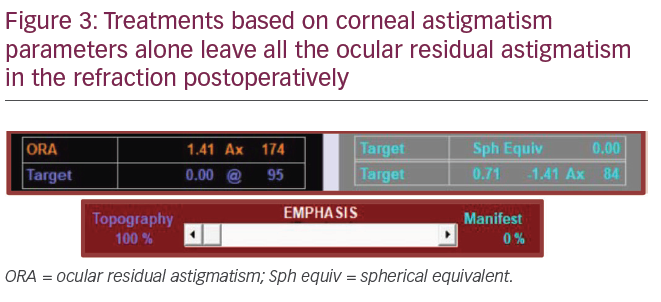
Using the example in Figure 1, the refractive cylinder (corneal plane) is -1.59 DC x 15 and the corneal astigmatism from CorT total is 2.80 D @ 95. The ORA is calculated as 1.41 D Ax 174. Once the ORA has been determined, what can be done about it? Ideally, when the magnitude and axis of the corneal and refractive astigmatism are the same, which is rare, then the ORA is zero and treating by refractive or corneal parameters alone would be appropriate. However, in most cases where this is not the case, treating by refractive parameters alone compared to incorporating Vector Planning will leave an excess amount of astigmatism on the cornea; that is, all the ORA (1.41 D) will remain on the cornea postoperatively (Figure 2). Conversely, treating by corneal astigmatism (topography-guided alone) will leave all the ORA in the refraction (Figure 3), often leaving the patient still requiring spectacle correction. The method of Vector Planning allows the surgeon to systematically treat the astigmatism anywhere on the 99 percentage points in between the two extremes of zero and 100%, with the aim of minimising the corneal and refractive astigmatism postoperatively and leaving the corneal astigmatism in a favourable and acceptable orientation such as with-the-rule. Previous studies have found the ‘sweet spot’ to lie at 60% emphasis on the ORA by refraction and 40% according to corneal parameters;5,6 however, this can be customised by the surgeon on a case-by-case basis, the preferred range lying between 50–65% to refraction.
It is important to note that the target corneal astigmatism (0.85 D @ 84) is aligned 90° away from the axis of the ORA (1.41 D Ax 174) to neutralise it, leaving the target refractive cylinder (–0.57 DC Ax 84) at the same positive axis as the ORA (Figure 1) to neutralise it. The target refraction is set to a spherical equivalent of zero, unless targeting monovision, so that the corneal astigmatism is reduced compared to treating by refractive cylinder parameters alone without increasing the refractive cylinder in practice. So not only is the corneal astigmatism reduced but the refractive cylinder is also reduced or the same as when treating by 100% refractive parameters.7 This can be related to the benefit of having a better shaped cornea, with less coma and trefoil, and with fewer complaints of associated symptoms.
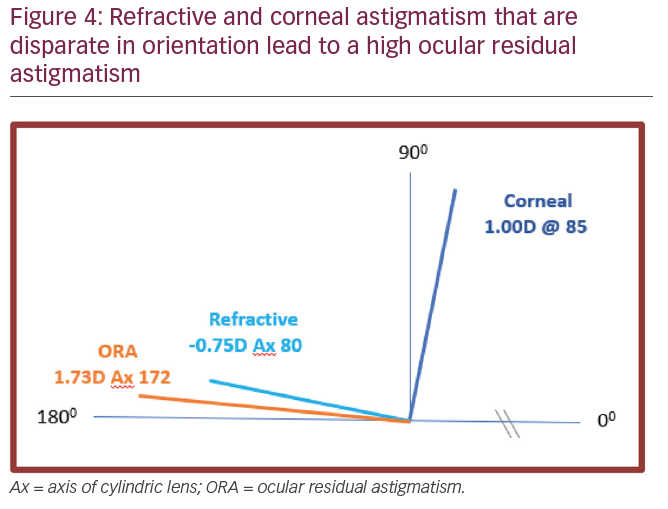
The method of Vector Planning also incorporates a safety mechanism whereby if the corneal astigmatism and the refractive cylinder are quite disparate (for example, the corneal astigmatism is 1.00 D @ 85 and the refractive cylinder is –0.75 D Ax 80; Figure 4), then treating a minimum amount of astigmatism or not treating any astigmatism at all will be planned, as treating either refractive or corneal astigmatism in preference will cause an excess of the other with a potential adverse effect. This is to avoid increasing the astigmatism magnitude postoperatively compared to the preoperative magnitude. There have been several studies using Vector Planning in refractive laser surgery,5,6 with the most recent one from Oman being the most significant in terms of a large cohort.7 The study by Dr Maria Arbelaez et al. used the Schwind Amaris excimer laser to treat 80 eyes using manifest refraction alone and 80 eyes with Vector Planning. Postoperatively the Vector Planning group had better visual results and less corneal astigmatism with similar refractive cylinder outcomes compared to the manifest refraction group.7
It is essential that, as corneal surgeons, we plan refractive laser procedures with the corneal as well as the refractive parameters in the treatment plan. Better measures of corneal astigmatism are now available to make its inclusion safe. After all, when planning toric intraocular lens procedures, it is the corneal astigmatism that is paramount in the selection of the most accurate implant to optimise astigmatic outcomes. Excimer laser refractive surgery similarly has a high priority for favourable corneal outcomes with a plano refractive result.
The Vector Planning calculator is freely available for trial on the ASSORT® website (www.assort.com). 


