




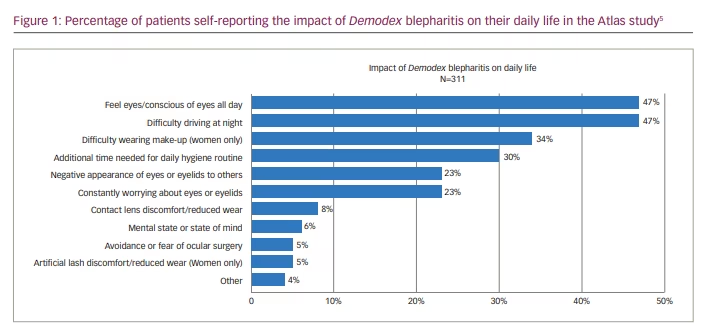
Demodex blepharitis is a highly prevalent lid margin disease that is commonly missed or misdiagnosed by eye care professionals. The disease is caused by an infestation of Demodex mites – tiny parasites that live in the eyelash follicles and feed on oily sebum. When present in small numbers, the effects of these mites are subclinical and are likely to go unnoticed. However, the mites may play a pathogenic role when their number exceeds some threshold, resulting in demodicosis.1 There are several plausible mechanisms by which Demodex mites contribute to blepharitis, including direct mechanical damage, acting as a vector for bacteria, and inducing hypersensitivity and inflammation.2–4 The infestation can also result in discomfort and psychosocial impacts (Figure 1).5 In advanced stages, the disease may impact the cornea and lead to epithelial erosions, infiltrates, defects and keratitis.6,7
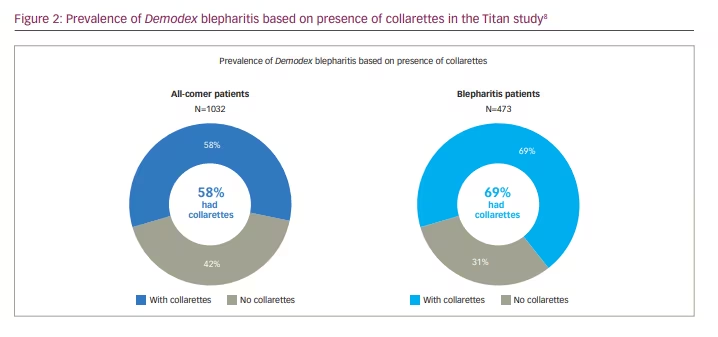
An estimated 25 million people in the USA have Demodex blepharitis,8–10 and data from the Titan study, presented at the American Society of Cataract and Refractive Surgery (ASCRS) 2021 Annual Meeting, revealed that more than two-thirds (69%) of blepharitis cases are associated with Demodex mite infestation (Figure 2).8 Although Demodex blepharitis can affect individuals of all ages, it has been established that the prevalence increases with age, with more than 80% of people who are 60 and 100% of those aged over 70 years presenting with the disease.4 Despite this high prevalence, many clinicians do not regularly screen for Demodex blepharitis. This is due to a variety of factors. First, the signs and symptoms of Demodex blepharitis often overlap with those of other ocular diseases, such as dry eye disease, so clinicians do not always see the true prevalence of Demodex blepharitis. Second, there are no medicines approved by the US Food and Drug Administration (FDA) for this disease, and evidence-based guidelines for the treatment of Demodex blepharitis are limited. The American Academy of Ophthalmology 2018 Preferred Practice Pattern for blepharitis outlines aetiologies and diagnosis of the disease but does not make recommendations on treatment beyond oral ivermectin, tea tree oil scrubs and microblepharoexfoliation.7 Topical ivermectin-metronidazole gel therapy has been tested with limited positive results, though specific symptoms such as itching, lid margin erythema and eyelash loss did not improve.11 Various products containing different concentrations of tea tree oil – in the form of gels, ointments, washes or lid wipes – have purported to demonstrate a reduction in signs and symptoms of blepharitis and in mite density in a minority of patients; however, the efficacy of these treatments in mite eradication remains unknown.12 These currently available Demodex management approaches typically result in poor patient compliance, increased patient frustration and, subsequently, worse patient outcomes. These options must also be used continuously and do not target the root cause of the disease – Demodex mites.
When left untreated, Demodex blepharitis can have serious, long-term impacts including severe inflammation in other eye structures such as the cornea, lash or lid abnormalities, and reduced quality of life. It is also well established that surgical patients – particularly the population undergoing cataract procedures – commonly have Demodex blepharitis.13 Fifty-six percent of cataract patients in the Titan study had Demodex blepharitis.14 Given the higher bacterial load in Demodex blepharitis patients compared with patients without the disease,15 minimizing the risk of bacterial infection prior to surgery by screening for Demodex blepharitis is also important.
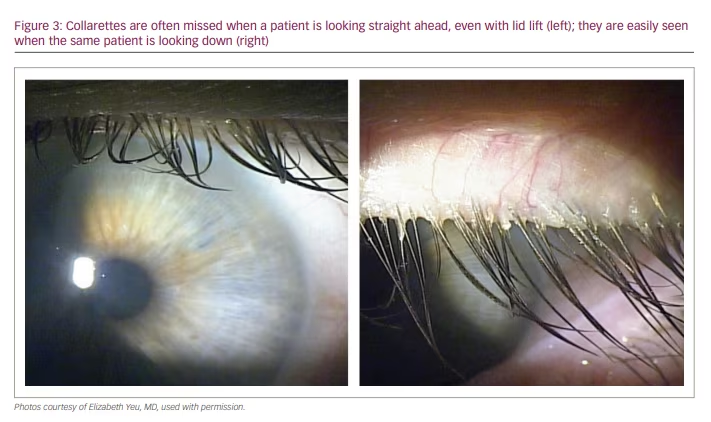
Finally, many eye care providers may not be aware that it is simple to screen for and detect Demodex blepharitis without any extra or special equipment. Collarettes, cylindrical waxy debris typically found at the base of the eyelashes, are the accumulation of mite waste and eggs and are the pathognomonic sign of Demodex blepharitis. Detecting Demodex blepharitis via the presence of collarettes can be incorporated into a routine slit-lamp examination by asking patients to look down while evaluating the upper lid margin for the presence of collarettes (Figure 3).
Owing to the suboptimal diagnosis and lack of efficacious, safe and tolerable therapies, patients continue to struggle. The Atlas study reported that over half of these patients (51%) have experienced signs and symptoms of Demodex blepharitis for more than 4 years, and 58% of patients were never diagnosed with blepharitis.16 This leads to frustration among patients and increases the burden on our healthcare system; we can do more to help these long-suffering patients.
The Titan study showed that approximately 58% of patients visiting eye care clinics for any reason present with collarettes.8 The Titan study findings are further supported by a prospective independent study presented at the Association for Research in Vision and Ophthalmology (ARVO) 2021 annual meeting,17 which found that demodicosis was newly diagnosed in 55.3% of patients, with 61.8% and 68.3% noted to have blepharitis and dry eye, respectively. These data illustrate that there is a significant opportunity to identify the disease sooner and potentially provide relief to more patients. While there has been a lack of effective treatment options to date, there is hope on the horizon.
A new investigational therapeutic, TP-03 (lotilaner ophthalmic solution, 0.25%; Tarsus Pharmaceuticals Inc., Irvine, CA, USA) is currently in development with promising data to date. Unlike existing treatments, TP-03 is designed to address the root cause of Demodex blepharitis – the infestation of the mites themselves. The active ingredient in TP-03 is lotilaner, an acaricide of the isoxazoline class and a well-characterized anti-parasitic agent designed to eradicate Demodex mites by selectively inhibiting insect, arachnid and parasite-specific gamma-aminobutyric acid chloride channels, leading to mite paralysis and death. It is also a highly lipophilic molecule, which may promote its uptake in the oily sebum of the lash follicles where the mites reside.
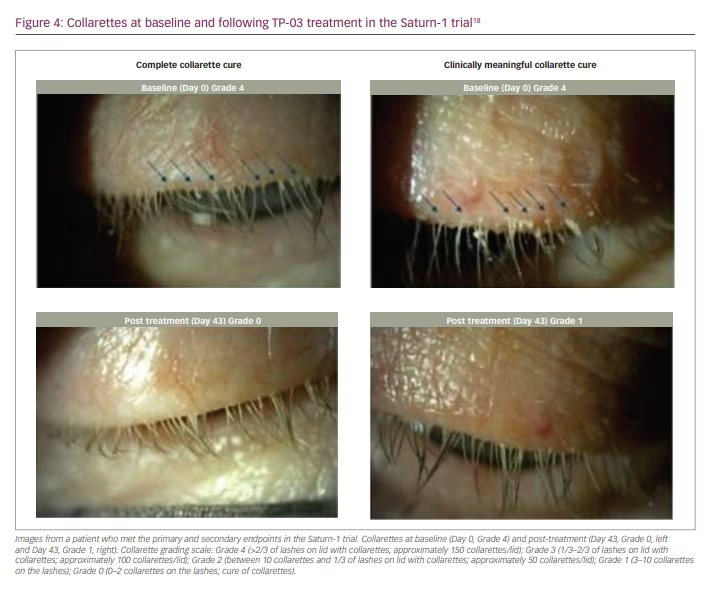
TP-03 is a multi-dose topical eye drop that has been evaluated in a phase IIb/III pivotal trial (Saturn-1), where it was dosed twice daily for 6 weeks in patients with Demodex blepharitis.18 In this study, TP-03 met all primary and secondary endpoints with high statistical significance when compared with vehicle, including complete collarette cure (defined as zero to two collarettes; primary endpoint), complete mite eradication (having zero mites; secondary endpoint), and composite cure based on complete collarette and erythema cures at Day 43 (secondary endpoint).18 The trial showed that TP-03 demonstrated complete resolution of Demodex blepharitis signs, had high responder rates, and was safe and tolerable. Furthermore, significant, clinically meaningful improvements were observed within 2 weeks across multiple endpoints (Figure 4). TP-03 also completely cleared lid redness (erythema) in one in five patients. The Saturn-1 trial was the first large-scale, randomized controlled trial to show positive, clinically meaningful and statistically significant results for a therapeutic specifically designed to treat Demodex blepharitis.
Earlier phase II studies of TP-03 in patients with Demodex blepharitis met their respective endpoints and demonstrated that TP-03 was effective in decreasing collarette grade and mite density, and was generally well tolerated with no significant adverse events.19,20
A second phase III pivotal trial (Saturn-2) with identical endpoints to those in Saturn-1 has completed enrolment with 412 patients, and I am one of the primary investigators for this trial.21 I am excited to participate in this trial because, for the first time, there is an investigational product that is designed to treat the root cause of Demodex blepharitis, a disease that has symptomatic and psychosocial impacts for so many individuals. TP-03 is an investigational drug that may help resolve the signs of the disease and alleviate the burden that it often places on patients’ daily lives and the overall healthcare system.
In addition to developing a safe and effective treatment for Demodex blepharitis, provider education, dialogue and in-office practices are also important and must evolve.
- All patients should be screened for Demodex blepharitis at every eye examination; providers need to evaluate a patient’s upper lid margin for the presence of collarettes by asking patients to look down during every slit-lamp examination.
- The long-term impact of untreated Demodex blepharitis must be discussed so that patients understand the need for therapy to potentially avoid worsening of the disease and long-term complications.
- Surgical patients should be treated in advance of their procedure when the presence of collarettes is detected, in order to avoid potential infection.
Demodex blepharitis is a disease that is often missed or misdiagnosed. As a result, many patients experience its negative impacts on a daily basis. Current methods for managing Demodex blepharitis produce variable efficacy and tolerability results and have not been tested in large-scale, randomized, vehicle-controlled studies. TP-03 (lotilaner ophthalmic solution, 0.25%) has demonstrated statistically significant elimination of collarettes, mites and redness in a pivotal trial. As we await an FDA-approved treatment for Demodex blepharitis, it is important to start screening and documenting all patients with this disease now so that we are best prepared to help our patients.


