




Presbyopia Correction – Outcomes and Personal Experience
Presbyopia correction is like the city that never sleeps; there is always something new on the horizon, yet currently available techniques have proven their capability to enhance the patient’s quality of life. Since the introduction of trifocal intraocular lenses (IOLs), presbyopia correction has been increasing around the globe. By now, there is a variety of different optical designs to improve the range of vision of our patients. While none of them are perfect, just like the human optical system, they have found their place in refractive and refractive cataract surgery. One of the latest introductions to the market is the enhanced depth of focus (EDoF) IOLs, which poses the question: aren’t all optical designs that compensate for the aging eye by offering a certain range of vision from distance to near, EDoF IOLs? The difference in general, seems to be the optical design rather than the marketing branding. Over the last 5 years, my team at Augentagesklinik Rheine and Greven (Germany) have continued the work I started at the University of Heidelberg, evaluating different optical designs to fulfil patients’ individual expectations for their vision. We decided to differentiate IOLs by their optical design, their range of focus and their possible side effects, rather than their marketing branding. This article is a short summary of our current findings, and the patient counselling process we employ to find the right IOL for each individual.
Full-range vision
For us, the definition of full-range vision is the ability to offer patients spectacle independence for distance, intermediate and near tasks. Still, there is differentiation between using bilateral trifocality with the same optical design, mixing and matching a combination of an intermediate-range IOL with a full-range IOL, performing a monovision approach with two intermediate-range IOLs. Several of our studies have shown good results and high degree of spectacle independency with bilateral trifocality.1–6 So far we evaluated several trifocal models, including the AT LISA® tri series (839MP and the toric 939MP; Carl Zeiss Meditec, Jena, Germany), the FineVision series (Micro F, POD F, POD F FT, POD F GF; PhysIOL, Belgium), the AcrySof® IQ PanOptix® (Alcon, Geneva, Switzerland), the Acriva Trinova (VSY Biotechnology, Istanbul, Turkey), the OPTIFLEX TRIO (Biotech, Luzern, Switzerland), the RayOne Trifocal (Rayner, West Sussex, UK) and the Alsafit Fourier (Alsanza, Pfullingen, Germany). We have long-term data up to 36 months for the AT LISA tri series, which shows high stability and efficacy with stable results for visual acuity, refraction and toric stability (Figure 1).
Regarding the comparison between those models, it is very difficult to make an objective evaluation. Despite that fact they are all trifocal IOLs, they vary by different add powers, light distribution for each focal point, filters and material. The preferred model is determined by the surgeon. Some offer slightly better intermediate range with less near range, and the implantation and axis alignment is material dependent. Generally, they all offer good results, especially when the optical, profile is matched individually to the patient’s expectations. Our true favourite, at present, is the combination of the AT LARA® series EDoF IOL (Carl Zeiss Meditec) or the TECNIS® Multifocal IOL +2.75 D (Johnson & Johnson, New Brunswick, NJ, USA) in the distance dominant eye, and a trifocal IOL in the near dominant (Figures 2 and 3).7,8 In our experience, this offers enhanced intermediate visual acuity with less dysphotopsia and still satisfying near vision.
Currently, we do not perform many monovision approaches, with one exception: if the patient clearly states they have no acceptance for dysphotopsia and understands the principle of monovision. In this instance, we follow the Duesseldorf scheme with the implantation of two Lentis® Comfort LS-313 MF15 IOLs (Oculentis, Eerbeek, Netherlands) while targeting the non-dominant eye on -1.0 to -1.5 D. This works exceptionally well, especially in patients that were used to an anisometropia without amblyopia, but also in myopes, and is another option in our variety of presbyopia treatments.
Low-range vision – the option with the least dysphotopsia
Low-range vision might be misleading for some doctors, but in our opinion, it is a bilateral implantation of the same optical principle with reduced light distribution to reduce optical side effects. This principle can be used to achieve stable and fluent vision of a defocus range of up to 2 D. In distance-focused candidates, we tend to create a smooth vision from distance to intermediate, while in near-focused candidates we target slight myopia (-0.75 to -1.25 D) to extend the range of vision from intermediate to near. Our latest data with the bilateral implantation of the AT LARA series has shown satisfactory results with less dysphotopsia compared to diffractive full range vision.7,9 Earlier work with the TECNIS Symfony® IOL (Johnson & Johnson) has also shown satisfactory distance and near visual acuity.10
Our current standard, for many years (if German medical insurance covers it), has been the bilateral implantation of the Lentis Comfort LS-313 MF15, targeting emmetropia.11 The rotational asymmetric profile and the low near addition of 1.5 D let the lens behave like a monofocal, regarding possible side effects, while offering the patient a range of vision from distance to an intermediate range of 70 cm (Figure 4). The alignment of the segment in an average person follows simple rules; most important, is that the visual axis goes through the distance optical part. This can be achieved by aligning the IOL to the Purkinje images by simply rotating it in the capsular bag. For the toric version, an upside-down implantation can also successfully solve the alignment. The same optical principle is now available on a hydrophobic C-loop platform (ACUNEX® Vario, Teleon, Leverkusen, Germany), offering similar outcomes with an additional blue-light filter implemented (Figure 5).
The most recent market introductions in this field are the xact™ Mono-EDoF™ (Santen, Japan), the TECNIS Eyhance (Johnson & Johnson), the Vivity™ (Alcon) and the IsoPure (PhysIOL). While the xact works with four diffractive rings, the achieved light distribution still adheres to the CE licensing of a monofocal IOL, achieving a range of vision from distance to 80 cm. Due to the close range of focal points and low amount of light distribution, dysphotopsia levels are as low as monofocal IOLs. The TECNIS Eyhance works with an optimised monofocal optic, and the Vicity with a wavefront optimised optic; both IOLs enlarge the range of vision without creating distinct focal points. These designs seem to be very promising, but are dependent on the individual optical properties of the human cornea. The IsoPure design is also related to the optical surface of the IOL, enlarging the range of vision without distinct focal points.
Take-home message
The variety of optical designs available for modern presbyopia correction provides countless opportunities for lens surgeons. There is not, and probably never will be, the perfect IOL for every individual, but there are many options for individualised patient care. This article is just a small overview, and does not cover all the options on the market or the global data that have been generated in the last decade. However, this article serves as a reminder to keep the anatomy of the individual eye in mind whilst considering all the options available to meet the patient’s expectations. Individualised eye care is here, and there are more options available on the horizon.
1: Visual acuity for distance, intermediate and near over a time period of 36 months with the AT LISA tri 839
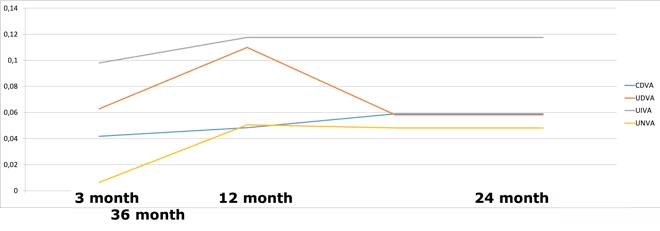
CDVA = corrected distance visual acuity; UDVA = uncorrected distance visual acuity; UIVA = uncorrected intermediate visual acuity; UNVA = uncorrected near visual acuity.
Figure 2: Theoretical range of vision with the ‘mix and match’ approach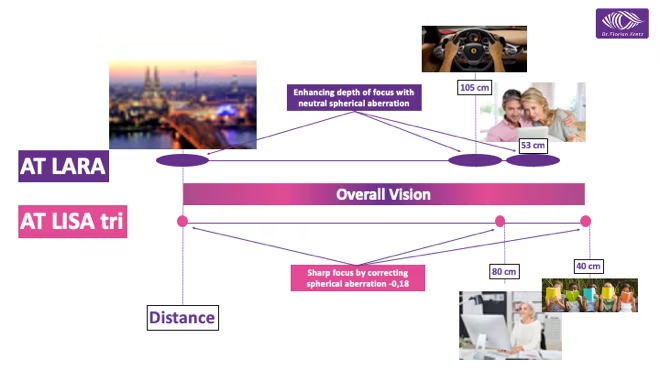
Figure 3: Monocular and binocular visual outcomes with the ‘mix and match’ approach in different distances
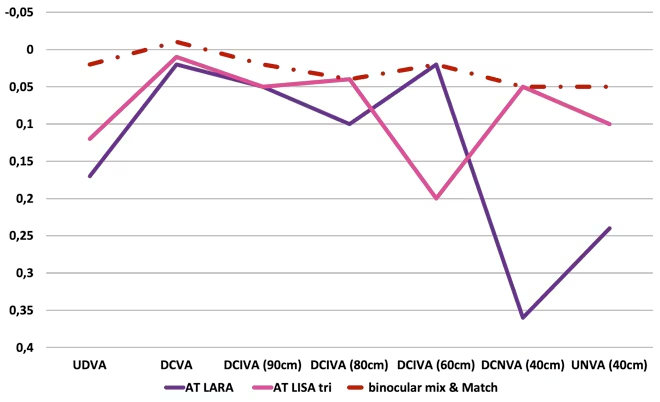
DCNVA = distance corrected near visual acuity; DCVA = distance corrected visual acuity; DCIVA = distance corrected intermediate visual acuity; UDVA = uncorrected distance visual acuity; UNVA = uncorrected near visual acuity.
Figure 4: Average halo and glare settings for bilateral implantation of Lentis® LS-313 MF15 Comfort (Oculentis, Netherlands)
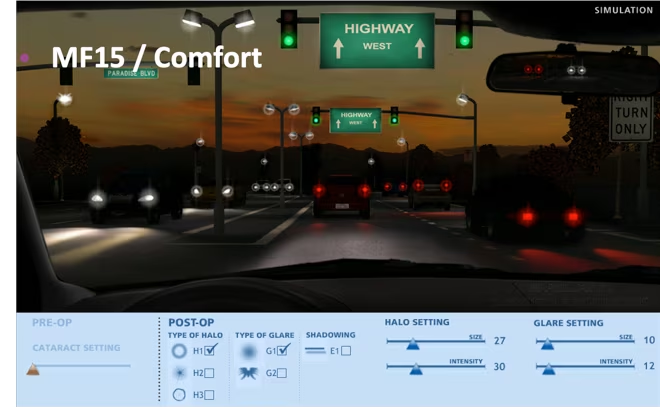
Figure 5: ACUNEX® Vario – hydrophobic, one-piece, c-loop, rotational-asymmetric intraocular lens with +1.5 dioptre near add-power (Teleon, Germany)
Disclosure: Florian Kretz reports grants, personal fees and non-financial support from Carl Zeiss Meditech, grants from Johnson & Johnson (AMO), personal fees from Polytech, personal fees from Vision Ophthalmology Group, personal fees from Rayner, grants from Hoya, grants from Santen, personal fees and non-financial support from Oculentis, personal fees from Bausch & Lomb, personal fees from LensAR, personal fees from Teleon, personal fees from Leica, personal fees from Bayer, and grants from Mynosis, outside the submitted work.
Support: Edited and supported by Touch Medical Media. No funding was received in the publication of this insight article.
Published: 27 November 2020