




A 34-year-old male presented to the clinic for a second opinion regarding ongoing symptoms of glare, ghosting, starbursts, haloes and reduced contrast sensitivity three years post-laser-assisted in situ keratomileusis (LASIK) surgery. These symptoms were exacerbated under low light conditions, particularly driving at night, and he found a reduction in their effect when shining his cell phone torch light in his eyes.
Preoperatively, manifest refraction was: right -3.25/-0.75 x 33, left -3.75/-0.50 x 152. His cycloplegic refraction was: right -2.50/-1.00 x 20 and left -3.00/-0.75 x 165.
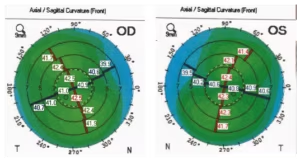
Simulated keratometry from topography preoperatively was: right 41.00/42.50 @ 102 and left 40.75/42.25 @ 75 with regular corneas in both eyes (Figure 1).
Pupil diameter under mesopic conditions was measured as: right 6.37 mm and left 6.94 mm.
Uncomplicated bilateral LASIK surgery was performed by another clinic in July 2016 using the latest generation Schwind Amaris® 1050RS Hz excimer laser (Schwind eye-tech-solutions GmbH & Co. KG, Kleinostheim, Germany) with the treatment based on the manufacturer recommended practice of manifest refraction only. The optical and the ablation zones were 6.70 mm and 7.63 mm, respectively.
At the 7-month postoperative review, unaided visual acuity was 20/20 part in both eyes and 20/15 with a manifest refraction of right plano/-0.75 x 9 and left plano/-0.75 x 170. Bilateral retreatment by flap lift was then performed based again on the manifest refraction, only because of the symptoms and remaining minor refractive error.
The patient attended our clinic 2 years post initial LASIK, complaining of significant symptoms of glare, ghosting, starbursts, haloes, and reduced contrast sensitivity (GASH), and wanted a second opinion on reducing these effects, which presented after the initial refractive laser surgery. On examination, the unaided visual acuity of right 20/20 and left 20/20-2 best correcting to 20/20 in both eyes. Manifest refraction right plano and left plano/-0.50 x 180. Cycloplegic refraction of right +0.25DS and left +0.50/-0.25 x 180. Corneal astigmatism using simulated keratometry from the CSO Sirius tomographer (C.S.O. Srl, Firenze, Italy), was right 1.12D @ 90 and left 1.04D @ 85. Ocular wavefront using the ViSX WaveScan system showed higher order aberrations of right 0.27 microns and left 0.40 microns.
It is interesting to note that there was still a significant amount (>1.00D) of corneal astigmatism remaining in each eye after both the first treatment and the second enhancements, which were based on the manifest refraction parameters alone. Treating the maximum amount of astigmatism by incorporating the corneal parameters into the refractive treatment plan employing Vector Planning1 would have left less corneal astigmatism postoperatively and reduced symptoms of glare, ghosting, starbursts, and haloes.
Figure 1: Preoperative axial curvature topography displaying regular with-the-rule astigmatism for right and left eyes
Ocular residual astigmatism
To treat the maximum amount of astigmatism, calculation of the ocular residual astigmatism (ORA) is required in each case. The ORA is defined as the vectorial difference between the corneal astigmatism and the refractive cylinder at the corneal plane.1 It is expressed in dioptres together with an axis and has been shown to be more than 1.00D in 46% of cases2 in one study and 34% of cases in another study.1
In this case, the ORA preoperatively was right 0.99D Ax 6 and left 1.24D Ax 174 (Figure 2). Due to the pre-existing corneo-refractive differences the ORA is the minimum amount of astigmatism that can remain postoperatively. Treatment based on the refractive parameters alone, as was the case here, would leave all the ORA, theoretically 0.99D @ 96 for the right eye and 1.24D @ 84 for the left eye to be directed to the cornea postoperatively. Note that this is 90 degrees away from the ORA axis to neutralise it. Even after the second treatment, which again was based on refractive parameters to reduce the refractive cylinder, there was still predictably a substantial amount of corneal astigmatism (>1.00D) remaining: right 1.12D @ 90 and left 1.04D @ 85 due to the significant amount of ORA.
Incorporating the corneal parameters into the refractive treatment plan after calculating the ORA would treat the maximum amount of astigmatism and leave less corneal astigmatism postoperatively compared to treatment based on refractive parameters alone with the same amount of refractive cylinder remaining.3 Vector Planning is a systematic method of combining both refractive and corneal parameters into the excimer treatment plan. This has been shown to reduce the corneal astigmatism remaining compared to treatments based on refractive parameters alone without compromising the refractive cylinder postoperatively.3
Vector Planning
The surgeon decides how to apportion the preoperative ORA calculated by placing an emphasis of corneal to refractive parameters anywhere from 1% corneal astigmatism and 99% refractive cylinder to 99% corneal and 1% refractive emphasis. Studies using the method of Vector Planning3–5 have shown 40% emphasis on corneal parameters and 60% emphasis on refractive parameters to be suitable for most treatments with a range anywhere from 45–65% emphasis by refractive parameters. The important consideration is the ORA, knowing that any emphasis on the ORA is treating the maximum amount of astigmatism.
Figure 2: The ocular residual astigmatism is calculated as the vectorial difference between manifest refractive cylinder at the corneal plane and corneal astigmatism
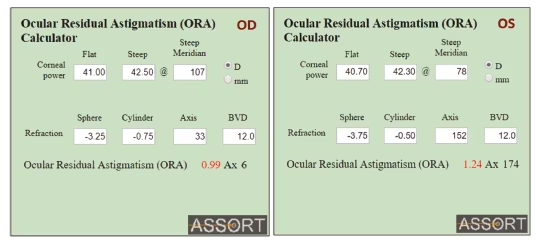
Figure 3: Calculation of ocular residual astigmatism for the right eye
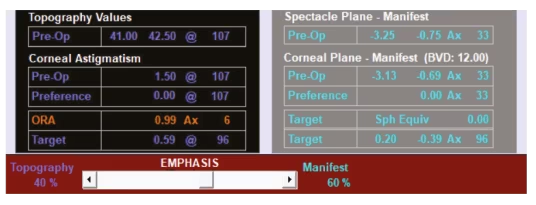
Applying Vector Planning to this case study, the ORA calculated for the right eye is 0.99D Ax 6. By emphasising, for example, 60% of the ORA towards refraction and 40% towards topography, 0.59D @ 96 would be targeted on the cornea and -0.39D x 96 in the refraction (Figure 3). This compares to 1.12D @ 90 of corneal astigmatism that the patient has postoperatively.
For the left eye the ORA is 1.24D @ 84. So again, emphasising the ORA by 60% towards refractive parameters and 40% by topography, the targeted corneal astigmatism would be 0.74D @ 84 and the refractive cylinder -0.50 x 84 (Figure 4). This compares to 1.04D @ 85 of corneal astigmatism that the patient now has postoperatively.
Vector Planning targets a spherical equivalent of zero in the refraction and because of the better corneal shape that the patient is left with postoperatively, compared to treatments based on refractive parameters alone, the targeted refractive cylinder has been shown not to be accepted by the patient in the postoperative manifest refraction.
Unfortunately, the patient did not want to undergo any further (third) surgery to reduce his symptoms, but was advised that Vector Planning was a viable option.
Excess corneal astigmatism is prevalent post refractive laser surgery with many complaints now documented in letters to the US Food and Drug Administration and the New York Times of symptoms of glare, ghosting, starbursts, haloes, or decreased contrast sensitivity, now commonly termed GASH6 as the acronym to describe these symptoms.
The method of Vector Planning can address the excess corneal astigmatism causing these disturbing symptoms and improving patient vision quality and satisfaction rates post-LASIK. The prevalence of these symptoms and signs together qualifies it as a syndrome. An ORA of more than 1.00D preoperatively and corneal astigmatism of greater than 1.00D postoperatively, together with any one or more of the GASH symptoms constitutes preventable avoidable LASIK surprise (PALS) syndrome. This syndrome is preventable by calculating the ORA preoperatively to ascertain how much corneo-refractive difference there exists. It is avoidable using the method of Vector Planning to reduce excess corneal astigmatism postoperatively, it can validly apply to photorefractive keratectomy and small incision lenticule extraction as well as LASIK procedures and the surprise of GASH can be minimized or eliminated by maintaining postoperative corneal astigmatism at less than 1.00D.
Laser manufacturers need to incorporate the Vector Planning method as a standard function of their laser systems, allowing all surgeons this option to maximally treat astigmatism and prevent PALS syndrome. This is currently not available on any laser. For surgeons who want to avail themselves of this facility of ORA calculation and Vector Planning with their refractive laser surgery, this is available as a free application at www.assort.com.⬛


