




Through the centuries, ceaseless innovation has advanced cataract surgery – the most frequently
performed operation on earth – from Daviel’s lens extraction, to Ridley’s intraocular lens (IOL)
implantation, to Kelman’s phacoemulsification, and now to femtosecond laser assisted techniques.1
Femtosecond laser surgery represents the marriage of two technologies: ocular imaging and laser
photolysis. Most lasers depend on intraoperative optical coherence tomography imaging. The
LENSAR™ femtosecond laser (LENSAR Inc., Orlando, Fl, US) utilizes proprietary augmented reality
(AR) imaging and anterior segment biometry based on scanning structured illumination. Super
luminescent diode technology provides the illumination for AR and scans at a variable rate depending
on the target structure, ensuring optimal contrast for structures with higher light scatter, such as
the cornea, as well as for those with little scatter, such as the posterior lens capsule. The 3D-AR
software locates anatomic interfaces including the pupil, anterior and posterior corneal surfaces and
the anterior and posterior lens capsule. The multiple images are collated using optical ray tracing
techniques to generate an exact 3D reconstructed model of the anterior segment.
In the LENSAR system, intraoperative imaging through structured illumination allows reconstruction
of a 3D model of the anterior segment of the eye, which is used to guide laser incisions.2 In addition
to intraoperative imaging, wireless digital communication technology now permits integration of
preoperative imaging into laser guidance. Recent US Food and Drug Administration (FDA) 510(k)
clearances have demonstrated the utility of linkage between preoperative diagnostic instruments and
the LENSAR laser, including the Cassini Corneal Shape Analyzer (Cassini, The Hague, The Netherlands),
the Corneal Analyzer OPD-Scan III (Nidek, Aichi, Japan), the Aladdin (Topcon Corporation, Tokyo,
Japan) and both the Pentacam® HR and the Pentacam® AXL (Oculus, Wetzlar, Germany). The key
to these linkages is iris registration, the accurate mapping and matching of iris features from the
preoperative image captured in the clinic to the intraoperative image captured through the laser
optics. Iris registration, based on high definition preoperative infrared images obtained with these
corneal diagnostic instruments, allows precise correlation of corneal topographic and total corneal
astigmatic data with laser treatment, opening the way for accurate correction of corneal astigmatism.
Correction of corneal astigmatism represents the entry point to refractive cataract surgery because
it is prerequisite to achieving spectacle independence for the majority of surgical candidates. The
introduction of toric multifocal and toric extended depth of focus IOL optical designs has raised
the bar for correction of astigmatism and presbyopia at the time of cataract surgery; however,
demonstration of the effectiveness of toric IOLs for correction of lower levels of corneal astigmatism,
particularly <1.00 D, has remained elusive. For example, approved labeling for the Tecnis® Toric IOL
(Johnson & Johnson Vision Care, Santa Ana, CA, US) states, “Study results
(residual refractive cylinder, change in cylinder, and uncorrected acuity)
stratified by preoperative keratometric cylinder did not show evidence of
significant benefit in the treatment of preoperative corneal astigmatism of
less than one diopter."3 Because uncorrected visual acuity can nevertheless
be compromised by mild astigmatism from 0.25 to 1.25 D, and because
approximately two thirds of candidates for cataract surgery have preexisting
corneal astigmatism in this range,4 corneal relaxing incisions and
arcuate keratotomies performed at the time of cataract surgery have
remained popular. While manual limbal relaxing incisions and arcuate
keratotomies have allowed reduction of mild to moderate pseudophakic
astigmatism,5 the advent of femtosecond laser arcuate incisions has
increased automation and standardization of treatment parameters.
However, few reports of the effectiveness of femtosecond laser arcuate
incisions in the context of cataract surgery have appeared in the literature.6
Even when utilizing the femtosecond laser, manual marking of the corneal
steep axis can introduce significant sources of error in the correction of
astigmatism. The same issues may arise, of course, with corneal marking
in preparation for alignment of toric IOLs. For example, in their recent study
of femtosecond laser arcuate incisions for the correction of astigmatism
at the time of cataract surgery, Chan et al. marked a single reference point
at the temporal limbus with the patient sitting upright to compensate
for cyclorotation. Once the patient was transferred to the femtosecond
laser platform, the temporal limbus was used as a reference point for
the zero-degree mark on a ring gauge. Nevertheless, these authors admit
“treatment misalignment was a major influential error-inducing factor in
astigmatism correction.”7
Accurate alignment of toric IOLs, and arcuate incisions, represents a critical
step in the correction of pre-existing corneal astigmatism. Not only has it
been estimated that there is 3.3% loss of effect for every degree of offaxis
correction,8 but it has also been suggested off-axis correction creates
a new vector resulting in abnormal induced astigmatism on an entirely
different axis, and induces higher order aberrations.9
Utilization of iris registration coupled with image-guided femtosecond laser
incision construction has the potential to improve accuracy and provide
superior refractive outcomes by overcoming the drawbacks of manual
marking techniques. LENSAR has developed Streamline technology with this
goal in mind, to permit accurate and reproducible reduction or elimination
of mild to moderate astigmatism in conjunction with femtosecond laser
assisted cataract surgery.
LENSAR with Streamline system
The acquisition of preoperative corneal topography, or total corneal
astigmatic analysis including the posterior corneal surface, with high
definition infrared digital images of iris features, forms the basis of imageguided
laser arcuate incision placement and construction. The corneal
diagnostic instrument can verify image compatibility at the point of
capture to minimize the risk of failure of cyclorotation compensation due
to the discovery of inadequate imaging once the patient is already in the
operating room. Streamline wirelessly transfers preoperative data from one
of the linked instruments (Cassini Corneal Shape Analyzer, OPD, Aladdin,
Pentacam HR or Pentacam AXL) to the LENSAR laser, reducing the number
of steps within the patient workflow and eliminating the need for staff to
transfer the correct data either manually or via a memory device.* At the
same time, wireless automated data transmission into the LENSAR patient
planning software eliminates potential transcription errors.
Iris registration is accomplished through selection and matching of iris
features from the preoperative, undilated pupil to the intraoperative,
dilated pupil.10 Streamline automatically corrects for cyclorotation after the
patient is docked to the laser, and does not necessitate that the surgeon
visually inspect and verify that cyclorotation compensation was accurate.
Streamline iris registration cannot be affected by loss of vascular detail due
to pharmacologic effects.
Arcuate incision planning software auto-populates incision parameters
based on the surgeon’s preferred nomogram and pre-programmed
surgically induced astigmatism (SIA). Arcuate incision planning can
automatically recommend laser incision placement based on preoperative
data; alternatively, there is the capability for manual entry or adjustment of
preoperative data. In addition, arcuate incision planning provides a graphical
interface to demonstrate SIA and calculated residual astigmatism. This
nomogram-based planning tool optimizes arcuate incision construction
by allowing modifications based on patient age and up to three additional
parameters, such as corneal white-to-white, central corneal thickness,
and corneal slope rate-of-change.
Multiple metrics can be customized to optimize arcuate incision planning;
these include incision depth, with options for fixed depth (250–900 μ), fixed
residual depth (0–300 μ), and percentage thickness (10–100%). ‘Against the
Rule’ and ‘With the Rule’ surgeon tables allow for entry of multiple data
points for arcuate incision length based on astigmatic power preferences.
Multiple data points can be added to better define arcuate incision planning,
such as single- or paired-arc treatments, modifiers, or surgeon preferences.
In addition, an age modifier provides the surgeon with the option to adjust
arcuate length utilizing an age-based chart. Finally, the incision placement
pop-up box allows the surgeon to adjust clear corneal incision (CCI)
locations preoperatively utilizing surgeon tables and SIA information in
order to minimize residual postoperative astigmatism.
Surgeons adopting LENSAR with Streamline arcuate incisions must
develop treatment nomograms and criteria for candidate selection.
While femtosecond laser arcuate incision nomograms have appeared in
the literature, nomogram development and refinement require tracking
and analyzing clinical outcomes.11 LENSAR with Streamline also has
demonstrated utility in the alignment of toric IOLs through the IntelliAxis™
corneal marking system (LENSAR Inc., Orlando, Fl, US), which produces
visible steep axis landmarks on the cornea that may be used by the surgeon
to verify the location of the steep axis relative to toric IOL orientation.
Clinical Results with LENSAR arcuate incisions
We have conducted a search of the published literature using PubMed.
gov, as well as relevant scientific meeting abstracts, using the search
terms “LENSAR” and “astigmatism,” in order to elucidate the safety and
effectiveness of LENSAR Streamline arcuate incisions. Several authors have
reported clinical outcomes with LENSAR with Streamline arcuate incisions.
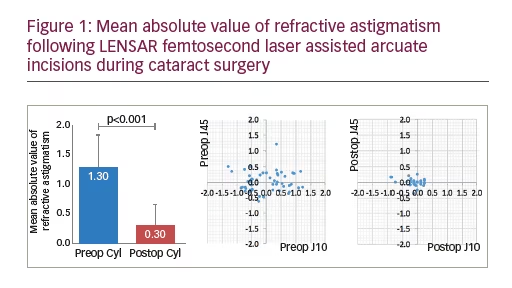
At the American Society of Cataract and Refractive Surgery 2016 Annual
Meeting, in New Orleans, Mitchell Jackson, MD presented data on 52 eyes
of 31 patients with pre-existing astigmatism ranging between 0.4 to 2.75 D.12
All patients underwent LENSAR femtosecond laser assisted arcuate
incisions during cataract surgery. A significant reduction in the mean
absolute value of refractive astigmatism from 1.3 D to 0.3 D (p<0.001),
was observed. Correspondingly, vector analysis of refractive cylinder also
revealed an improvement in the J0 and J45 vectors. No complications were
observed (Figure 1). The author concluded that LENSAR laser assisted
astigmatism correction by arcuate incision construction during cataract
surgery, is a safe and effective treatment option.
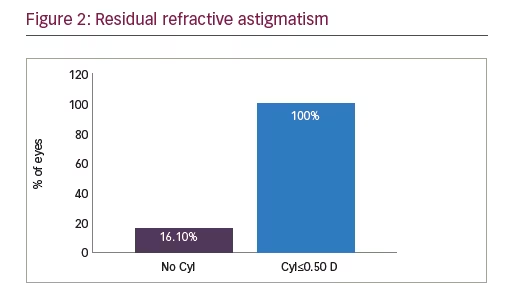
Also at the at the American Society of Cataract and Refractive Surgery
2016 Annual Meeting in New Orleans, Jonathan Solomon, MD presented
data on 31 eyes with regular corneal astigmatism treated with the LENSAR
laser with Streamline, to perform partial thickness arcuate incisions with
implantation of a monofocal IOL.13 Postoperatively, 90.3% of eyes were
within 1.00 D and 83.9% of eyes were within 0.50 D of the spherical
equivalent target refraction. 100% of eyes achieved postoperative refractive
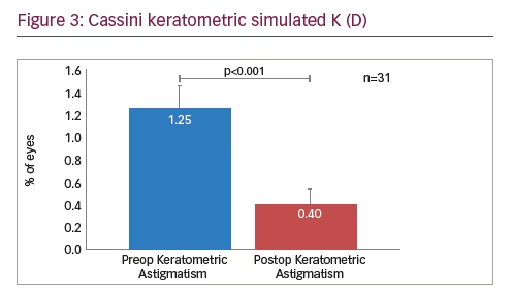
astigmatism ≤0.50 D (Figure 2). In addition, corneal simulated keratometric
astigmatism as measured by the Cassini Corneal Shape Analyzer was
reduced significantly from a preoperative mean of 1.25 D to 0.40 D
postoperatively (Figure 3).
The author concluded that precise and reproducible arcuate incisions can
be constructed with the LENSAR laser.
At the American Society of Cataract and Refractive Surgery 2017 Annual
Meeting in Los Angeles, Denise Visco, MD presented a retrospective
study comprising data from 279 eyes of 203 patients with cataract
and pre-existing keratometric astigmatism ranging from 0.50 D to 1.91
D.14 All eyes underwent LENSAR femtosecond laser assisted cataract
surgery and arcuate incision construction using Streamline wireless
transfer of the preoperative undilated iris registration image and corneal
astigmatism data from the Cassini Corneal Shape Analyzer. Cyclorotation
was automatically compensated by adjusting incision placement, and the
incision parameters were automatically generated by the LENSAR arcuate
incision planning software based on the surgeon entered nomogram and
personalized surgically induced astigmatism.
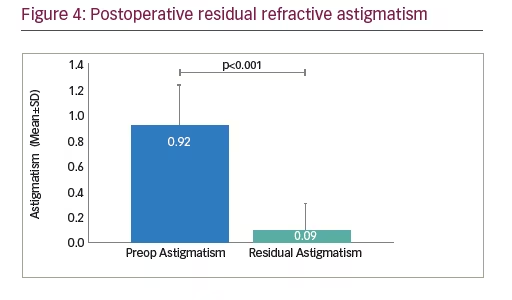
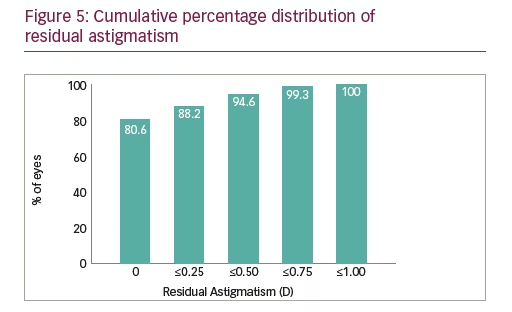
The primary outcome measure was postoperative residual refractive
astigmatism. Preoperatively, mean keratometric astigmatism measured
0.92 ± 0.33 D; postoperatively, mean refractive astigmatism measured 0.09
± 0.21 D (Figure 4). 94.6% eyes had ≤0.5 D and 99.3% eyes had ≤0.75 D
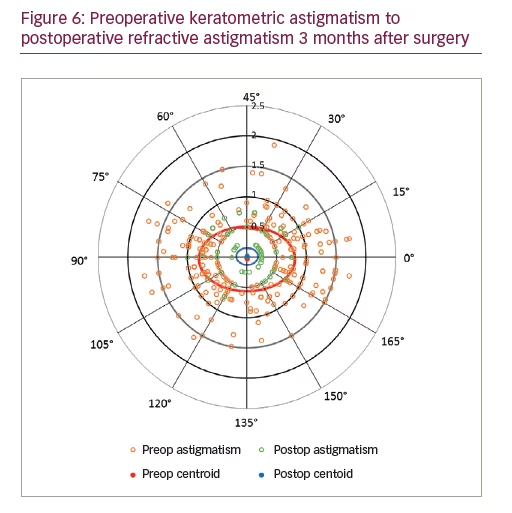
residual refractive astigmatism (Figure 5). A double angle plot graphically
demonstrates significant reduction of preoperative keratometric
astigmatism to postoperative refractive astigmatism 3 months after
surgery (Figure 6). There were no intraoperative complications. The author
concluded that LENSAR with Streamline arcuate incision planning software
using iris registration yielded safe and effective outcomes in cataract
patients with low to moderate astigmatism.14
Discussion—LENSAR arcuate incision
clinical outcomes
These results, demonstrating 94.6–100% of eyes ≤0.50 D residual
refractive astigmatism, compare favorably with published outcomes of
femtosecond laser arcuate incisions performed at the time of cataract
surgery, utilizing other laser platforms. In their study of 51 eyes of 37
patients operated with the LenSx® laser (Alcon Laboratories, Inc., Fort
Worth, TX, US), with mean preoperative keratometric astigmatism of 1.45
± 0.44 D (range, 0.50–2.50), Wang et al. reported 50% of eyes ≤0.50 D
residual refractive astigmatism at 3 months postoperative.15 Day et al.
reported 32.1% ≤0.50 D residual refractive astigmatism in a cohort of 196
eyes of 133 patients, with mean preoperative keratometric astigmatism
of 1.21 ± 0.42 D (range, 0.75–2.64) operated with the Catalys® laser
system (Johnson & Johnson Vision Care, Santa Ana, CA, US).6 In their
study of 54 eyes of 54 patients with mean preoperative keratometric
astigmatism of 1.33 ± 0.57 D (95% confidence interval [CI], 1.31–1.35),
Chan et al. performed arcuate incisions using the VICTUS® laser
(Bausch & Lomb, Dornach, Germany) and reported 33% of eyes ≤0.50 D
residual refractive astigmatism.16 The higher means and upper limits of
preoperative keratometric astigmatism of eyes enrolled in these studies
may have impacted postoperative residual refractive astigmatism,
and the outcomes suggest that eyes with >2.00 D pre-existing corneal
astigmatism are likely better candidates for toric IOL implantation. Visco’s
study highlights the most effective range of femtosecond laser arcuate
incisions, from 0.50 D to 2.00 D preoperative keratometric astigmatism.14
In addition, utilization of iris registration for accurate placement of
incisions likely reduces error from misalignment. As Chan et al. point out,
“The variability in treatment alignment can be the result of inconsistency
in aligning the steepest meridian to the incisions.”16
Clinical results with LENSAR IntelliAxis toric
IOL alignment
For those patients with moderate or greater astigmatism not likely to be
completely corrected by arcuate incisions alone, toric IOLs offer a proven
refractive option. As mentioned above, LENSAR with Streamline includes
the capability of marking the corneal steep axis with IntelliAxis based on
wireless transmission of preoperative diagnostic data and iris registration
in order to provide landmarks for toric IOL alignment.
Visco and Weinstock presented results of a multicenter, prospective,
non-masked clinical study including subjects having astigmatism with
cataracts desiring lens extraction and toric IOL implantation.17 Other
inclusion criteria were keratometric cylinder between 0.75 D and 4.50 D
and successful iris registration for cyclorotation compensation. All
subjects in the study underwent LENSAR laser assisted cataract surgery,
with the creation of steep axis corneal landmarks (using intrastromal
corneal incisions), followed by toric IOL implantation. Toric IOLs were
aligned rotationally using the femtosecond steep axis landmark. The
subjects were followed at 1 day and 1 month, postoperatively. Seventythree
eyes were enrolled in the study with a mean preoperative corneal
cylinder of 2.23 ± 0.19 D (range, 1.15–4.5 D). Postoperatively, at one month,
93.2% of eyes achieved ≤0.50 D and 76.7% of eyes achieved ≤0.25 D
residual refractive astigmatism. The mean residual refractive astigmatism
was 0.19 ± 0.38 D. These results compare favourably with other studies of
toric IOL implantation.18
Stephenson presented results of a prospective comparative study in which
axis marks based on Cassini Total Corneal Astigmatism (TCA; Cassini,
The Hague, The Netherlands), which captures both anterior and posterior
corneal cylinder, were placed with the LENSAR femtosecond laser IntelliAxis
system.19 Intraoperative aphakic measurements were obtained using the
ORA™ intraoperative aberrometer (Alcon, Ft. Worth, TX). Vector analysis
was used to calculate the difference between preoperative total corneal
astigmatism, femtosecond-guided corneal marks and intraoperative
aberrometry-measured astigmatism. Results included data on 74 eyes of
47 subjects undergoing toric IOL implantation. Measurements of corneal
astigmatism preoperatively by Cassini TCA and intraoperatively by ORA
were highly correlated: Pearson correlation coefficients (R) for axis and
magnitude of corneal astigmatism were 0.94 D and 0.72 D, respectively (p<0.0001 for each). The author concluded that the correlation between
preoperative and intraoperative measurements provided a high level of confidence in selection and alignment of toric IOLs.
Approach to the patient
Correction of astigmatism is fundamental to refractive cataract surgery.
Whether utilizing arcuate incisions for mild astigmatism or toric IOLs
for moderate and higher astigmatism, accurate alignment represents
a critical step in achieving the full intended correction. Image guided
laser incisions and corneal marks for toric IOL positioning, based on
preoperative corneal analysis and iris registration, provide highly
precise guidance for alignment of astigmatic correction. Nomogram
development and adjustment based on postoperative outcomes allow
for continuous improvement.
Informed consent at the time of cataract surgery requires discussion of
alternative procedures, including refractive correction of astigmatism.
Reduction or elimination of spectacle dependence has become a widely
understood option for cataract patients. Multiple methodologies are
offered in practice today, ranging from monovision with arcuate incisions
to bilateral toric extended depth of focus IOLs. Corneal refractive
procedures continue to find utilization for enhancement of residual
refractive error.20 Given the complexity of the available options, clear
and concise communication with patients has become an essential
component of refractive cataract surgery.
From the patient’s perspective, there are three options for needing
glasses in order to see things clearly: none, single vision glasses, or
(usually progressive) bifocals. Image quality can be difficult to explain,
but it is most often discussed in terms of the “halos around lights”
that accompany multifocal or extended depth of focus IOLs. Through
interaction with the patient, the surgeon must determine the patient’s
degree of motivation for spectacle independence and relative tolerance
for unwanted optical side effects, i.e., dysphotopsia and reduced contrast
sensitivity. From this assessment should spring a recommendation for
the most likely successful technological approach, which should then
be explained in as simple a way as possible. Regardless of the decision,
clinical results to date show that there may be significant benefit to
offering correction of mild astigmatism via femtosecond laser arcuate
incisions. The results obtained, and the potential for further improvement
through ongoing nomogram adjustment, make this modality an
extremely promising route towards spectacle independence.


