




Spotlight interview with Cynthia Matossian on the impact of COVID-19 on her practices

Cynthia Matossian is the founder and medical director of Matossian Eye Associates, a practice with three offices in Pennsylvania and New Jersey. She is a consultant to numerous pharmaceutical and medical device companies and is on the leadership team of the American College of Eye Surgeons, the NY IOL Implant Society, and Women in Ophthalmology. She serves on multiple editorial boards, has published numerous articles, and received the prestigious Ophthalmic World Leaders Visionary Award and was included in the Ocular Surgery News’ Premier Surgeon 300 list. She is a Clinical Assistant Professor of Ophthalmology (Adjunct) at Temple University School of Medicine.
Q. Please describe the impact of COVID-19 on your practice of ophthalmology?
COVID-19 brought all elective cataract surgery to an immediate halt. It was the first time ever, to our collective recollection, that no elective cataract surgery was performed anywhere in the US. Our practices were open for urgent and emergent patients with only a skeletal crew. The rest of our staff was furloughed. The decision to furlough staff, knowing that some live paycheque-to-paycheque, was emotionally very difficult. Our HR department was available to help answer staff questions regarding unemployment paperwork or assist them with questions relating to health insurance benefits. Our clinic volume dropped precipitously to about 15%.
COVID-19 has catapulted us to using a technology that was available but one we had not yet incorporated into our practice. Telemedicine has proven to be one of the most important tools to communicate with patients during these shelter-at-home times. Through the digital medium of ZOOM, we can help both new and established patients. It turns out to be a good screening tool for red eyes, chalazia, and dry eye disease. Even for glaucoma patients on chronic eye medicines, a telemedicine call helps reinforce compliance.
New standard operating procedures are being tweaked on a regular basis. Patients can complete as much of the registration process as possible via a telephone call to minimise their throughput time in our office. All our staff, doctors and patients are wearing masks and we provide patients with a mask if they do not have one upon arrival to the office. We have ordered larger slitlamp shields for enhanced protection for both the patient and the medical staff. In the past, we encouraged family members to join our patients in the exam room. Unfortunately, we are limiting the exam to patients only unless the patient needs assistance.
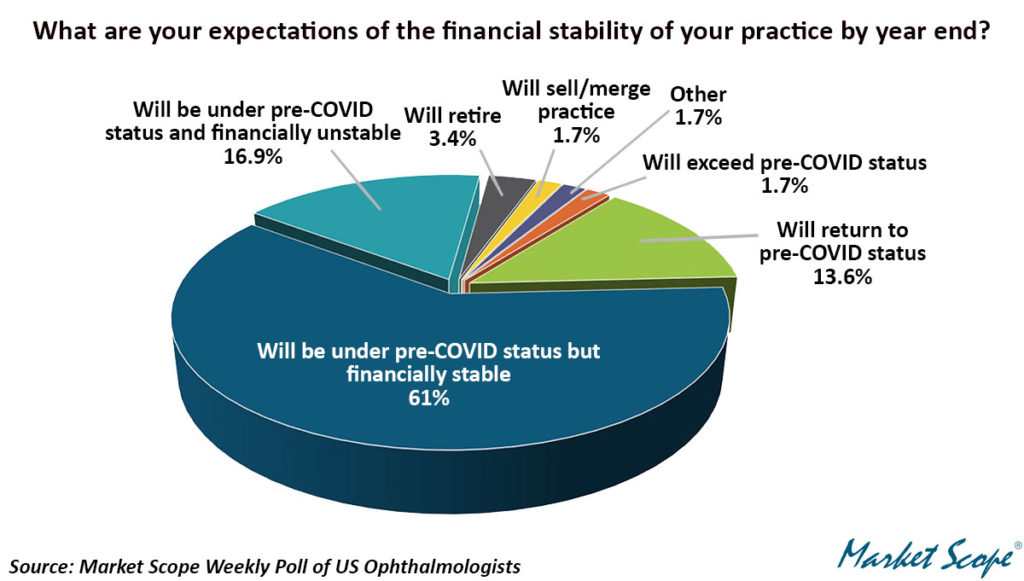
Temperature checks for staff, physicians and patients will be mandatory upon entering the office. For staff and doctors, it may be repeated at midday. Our reception room has chairs spaced 6 feet apart and temporary plexiglass dividers around our front desk receptionists. We are asking patients to remain in their car until they receive a text to come in. We plan to start with about 25% capacity and increase this number as we master our new processes and hone our patient flow. Our templates may have to be reduced to 3 patients per hour to include frequent cleaning of equipment and diagnostic surfaces in between every encounter. Our goal is to achieve 50% pace as soon as feasible then gradually increase our capacity without compromising safety. Please see below a recent Market Scope survey stating that over 70% of respondents will be negatively affected by the Corona virus situation.
There is light at the end of the tunnel. Shelter at home recommendations are loosening and rules are becoming more relaxed. Retail businesses, restaurants and brick and mortar stores will be hit hard, but everyone values their vision. It is not expendable; it is prioritised and highly valued.
Q. How did you spend your time during the shelter at home period?
The time during shelter at home was helpful and restful, but also stressful. I caught up on work, sleep, emails, my journal reading, and I participated in countless webinars and led or moderated multiple educational webinars or digital events. I worked out every day, cooked leisurely and ate healthy meals at home with my husband. I feel physically fitter and stronger, but emotionally somewhat hurting since I miss the human interaction with my patients, staff, family, colleagues and friends. I miss hugs and handshakes.
I believe there will be a hybrid medical practice landscape going forward. The digital portion with telemedicine is here to stay and predicted to grow. These tele-ophthalmology visits may be ideal for LASIK and oculoplastics post-op visits, for dry eye follow up visits or to screen “red eye” calls. The in-person in-office exams will focus on elements that can only be completed in the office.
Q. What changes that were instituted during COVID are going to stay after the practice doors reopen?
– More intense hygiene protocols at every step
– Telemedicine at the forefront of clinical practice
– Separate testing rooms to accommodate one diagnostic/treatment piece of equipment
– Shorter in-office patient transit times
– An increase in home working for certain departments such as billing, pre-certification, pre-registration and marketing
Q. How do you think COVID-19 has impacted your patients when it comes to scheduling their visit with their eye doctor?
Patients have really appreciated the convenience of telemedicine – not having to drive to the office, get dressed up, find and pay for parking (where applicable), and they have loved getting to the virtual appointment without any of the typical wait time delays before interacting with the doctor. My patients have felt very appreciative of our effort to reach out to them and devote one-on-one and face-to-face time through Zoom. For those who do not have a laptop, iPad or a device to accommodate telemedicine, I have telephone call appointments with great success.
Q. Challenges create opportunities: how to make the best lemonade from lemons
Dry eye lends itself very well to telemedicine. It provides one on one uninterrupted, undistracted time to help the patients and physicians connect in a meaningful way.
– Reviewing compliance with the patient by the physician rather by a technician has proven to be ‘eye opening’. Patients appear to be more honest with their compliance challenges with their dry eye treatment protocols. Many patients have a multi-tier daily treatment to which they are expected to adhere. What % of patients are accurately compliant?
– Some non-compliance stems from lack of understanding of how best to use the product or how best to perform a recommended procedure. Other contributors to non-compliance are the lack of overall understanding of the underlying chronicity of their dry eye disease state.
– Explanation to patients, I believe, needs to take many forms: written, verbal and perhaps via a post visit follow-up telemedicine interaction. Patients have different questions to ask once they try a drop or a procedure at home, which they would not have known to ask in the office before starting.
– Environmental observations: During Telemedicine, I noticed that about half of the patients with whom I spoke had ceiling fans. None were in motion since it is still cool these days in Pennsylvania and New Jersey. However, if these fans are above the patient’s bed or blow into their eyes, this will exacerbate the patients’ dry eye disease. Asking them to not use the fan when they are in the room would not have come up in an office setting since we do not typically query patients about fans and air vents blowing towards their eyes/face.
– Via telemedicine, we can ask to observe a patient putting drops into their eyes and provide tips on how to be more effective at this task.
– Telemedicine is here to stay – the landscape is ever changing and it will take patients, insurance carriers and physicians time to work out the details of how best to use this tool.
Support: Commissioned, developed and supported by Touch Medical Media.
Published: 13 May 2020