




Glaucoma is a multifaceted disorder resulting from damage to the retinal ganglion cells (RGCs) and their axons, causing progressive optic nerve degeneration and leading to irreversible blindness in some patients.1–4 In most cases the condition develops gradually, with peripheral vision loss typically being followed by loss of central vision.5 In the US, in 2011, openangle glaucoma (OAG) affected 2.71 million persons and is estimated to rise to 7.32 million by 2050.6 Globally, glaucoma affected an estimated 64.3 million people (aged 40–80 years) in 2013.7 Given the aging of the world’s population, this number is expected to rise to 76.0 million in 2020 and to 111.8 million in 2040.7
Ocular hypertension (OHT) can be defined as a high intraocular pressure (IOP) without observable optic nerve damage.4 OAG and angleclosure glaucoma are the two predominant types of glaucoma, and are characterized by an elevated IOP.9 Normal tension glaucoma (NTG) is a form of OAG that is prevalent in both Japanese and Western populations.10 While damage to the optic nerve occurs without elevation of IOP in NTG, IOP reduction has been shown to reduce visual field damage in patients with NTG.10
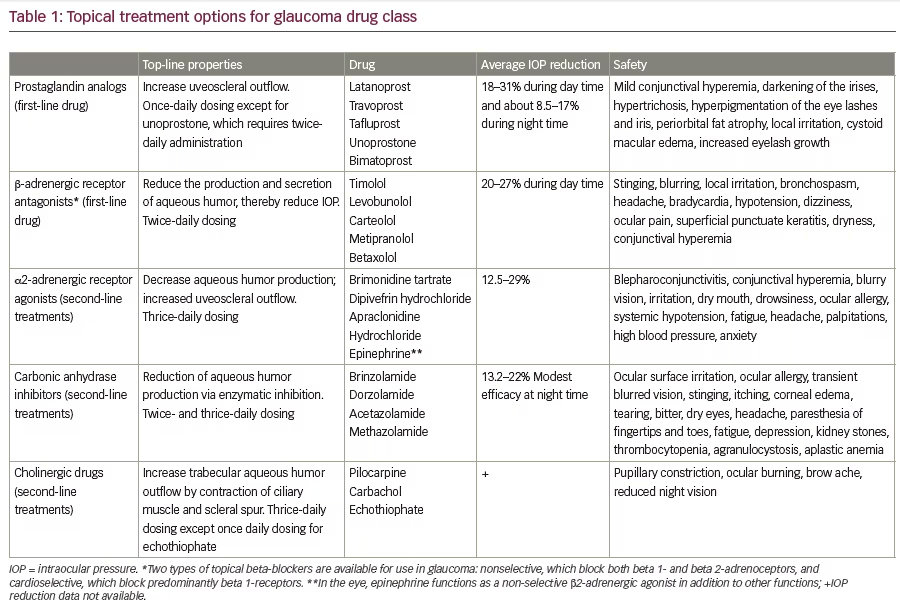
Current treatment options target IOP reduction to delay progressive glaucomatous damage and to delay onset of visual field loss in subjects with OHT; these include topical medications, laser trabeculoplasty, and surgical drainage procedures (micro-invasive glaucoma surgery [MIGS], trabeculectomy, tube shunts).11–13 However, commonly used topical treatments (prostaglandin analogs [PGA], beta blockers, carbonic anhydrase inhibitors, and α2-adrenergic agonists) can be limited by ocular and systemic side effects, allergies, the need for multiple administrations every day, poor adherence/compliance, and an inability to consistently control 24-hour IOP (Table 1). A new molecular entity incorporating both the established prostaglandin F2α (PGF2α) analog, latanoprost acid and a nitric oxide (NO)-donating group (latanoprostene bunod [LBN, BOL-303259-X] Bausch & Lomb Inc. Bridgewater, NJ, USA) is currently under review by the Food and Drug Administration (FDA) in the US as a novel IOP-lowering monotherapy for glaucoma management. This review discusses the dual mechanism of action of this potential new treatment and evaluates the clinical evidence supporting the compound’s efficacy.
Pathophysiology of glaucoma
Increased IOP raises risk for glaucoma, which is characterized by RGC damage and death that results in changes to the optic nerve head and the visual field. IOP is affected by the balance between aqueous humor (AH) secretion and its subsequent drainage through the trabecular meshwork (TM) and the uveoscleral outflow pathway.5,14–17 AH is secreted into the anterior chamber via the ciliary epithelium and returns to the vasculature through the TM into Schlemm’s canal, draining into collector channels, aqueous and episcleral veins; or it is drained via the uveoscleral route. Recent laboratory studies show cyclic IOP changes, possibly prompted by a reduction in pressure-dependent drainage, alter this aqueous outflow.18 At least 75% of the resistance to AH outflow in humans is localized within the TM, predominantly in the juxtacanalicular portion; in glaucoma, this tissue is altered leading to elevated IOP.16 In addition to IOP, other risk factors affecting the development and/or progression of glaucoma include older age, African ancestry or Hispanic ethnicity, larger optic nerve cup-to-disc ratios, thinner central corneas, family history of glaucoma, diabetes, myopia, history of migraine headaches, and lower ocular perfusion pressure.19,20
Current medical treatments for glaucoma
Topical ocular hypertensive medications which lower IOP have been the mainstay for first-line treatment of OHT and OAG to even before large, population-based clinical studies identified IOP as a modifiable risk factor. The Ocular Hypertension Treatment Study evaluated 1,636 individuals with an IOP of 24–32 mmHg in one eye and 21–32 mmHg in the fellow eye who were randomized to observation or to topical ocular hypotensive medication.21 Early treatment of OHT to lower IOP decreased the cumulative incidence of OAG at a median follow up of 13 years (16% versus 22% overall; p=0.009).
The Early Manifest Glaucoma Trial was a randomized clinical trial that included 255 patients aged 50–80 years (median, 68 years) with early glaucoma, visual field defects (median mean deviation, -4 dB), and a median IOP of 20 mmHg.11 These signs were mainly identified through a population screening. The patients were randomized to no initial treatment or to treatment. The treated patients had laser trabeculoplasty and started receiving topical betaxolol twice daily in eligible eyes. Follow-up visits included tonometry and computerized perimetry every 3 months and fundus photography every 6 months. The results suggest that a reduction of 1 mmHg could be correlated with an approximate 10% decrease in risk for glaucoma progression over a 4–6 year period.11,12 There are five major classes of topical medications currently approved for the treatment of elevated IOP designed to either reduce the production of ocular fluid or facilitate its outflow (Table 1).22–24Until the pathophysiology of glaucoma is better understood, there is little likelihood other therapeutic targets will become a more central component of glaucoma management. Each of these classes of drugs has its own advantages and drawbacks (Table 1). The α2-adrenergic receptor agonists, for instance, decrease the production of aqueous by the ciliary body and act on uveoscleral outflow, but can cause fatigue, high blood pressure or anxiety. While the β-blockers reduce AH secretion to lower IOP, and although rarely cause ocular side effects, may cause respiratory and cardiac side effects.22,23 Also, unlike the cholinergics, β-blockers do not affect pupil size. As miotics, the cholinergic agents target the conventional outflow pathway indirectly, by inducing ciliary muscle contraction that expands the TM and dilates Schlemm’s canal, reducing outflow resistance; however, they are not used widely due to local side effects.25
The side-effect profile of the PGA class of drugs is substantially superior to that of the β-blockers, which meant that the class quickly became the first-line treatment of choice for many clinicians. This class of drugs is known to cause conjunctival hyperemia,26 but the effects are typically considered mild and transient. Other effects include permanent iris color change and periorbital pigmentation and eye lash growth.27 PGAs bind primarily to prostaglandin receptors in the TM, ciliary muscle, and sclera, leading to altered matrix metalloproteinases expression.17,28 The mechanism of action of this class enhances uveoscleral outflow to lower IOP. The first PGA to be approved was latanoprost, and since then other PGAs, including travoprost, tafluprost, bimatoprost, and unoprostone, have also received regulatory approval.29
New and emerging glaucoma treatments
Several new IOP-lowering treatments that target various other mechanisms of action are in late-phase development. Among them is netarsudil (Rhopressa™, AR-13324 [Aerie Pharmaceuticals, Inc, Irvine, CA, US]) ophthalmic solution, which is a small-molecule inhibitor of both Rho-kinase (ROCK) and the norepinephrine transporter (NET). Netarsudil is thought to target the trabecular network and thus the abnormal tissues responsible for elevated IOP in glaucoma. The safety and efficacy of netarsudil monotherapy are being compared with timolol maleate (0.5%) in patients with OAG or OHT in two phase III trials (NCT02246764 and NCT02207621, n=240 and 690, respectively). A phase II clinical trial (n=298) showed that in patients with OAG or OHT, a fixed combination of netarsudil 0.02% and latanoprost (0.005%) (Roclatan®, PG324 [Aerie Pharmaceuticals, Inc, Irvine, CA, US]) showed significantly improved reduction in IOP than either of the two treatments alone (p<0.0001).30 The most frequently reported adverse event was conjunctival hyperemia, which occurred with an incidence of 41% (30/73), 40% (29/73) and 40% (31/78) in the PG324 0.01% and PG324 0.02% and AR-13324 0.02% groups, respectively compared with only 14% (10/73) in the latanoprost group.
Another class of potential IOP-lowering agents is the adenosine agonists. These bind to adenosine A1 receptors which, in the eye, reduce outflow resistance consequently lowering IOP.31 An example is trabodenoson (INO- 8875), which showed significantly greater reductions in IOP compared with placebo at 14 and 28 days (p=0.01 and p<0.001, respectively) in a phase II trial of patients with primary open-angle glaucoma (POAG) or OHT.32,33 The effect on IOP and safety parameters of trabodenoson at three different dose levels (4.5% twice daily [BID], 6.0% once daily [QD], 3.0% QD), timolol 0.5% BID, and placebo is being compared in a phase III trial in patients (planned n=335) with POAG and/or OHT (NCT02565173).
A3 adenosine receptor (A3AR) agonists have been found to protect normal cells from undergoing apoptosis via the downregulation of death signals and may be able to prevent RGC apoptosis.31 A phase II study on an oral A3AR medication, CF-101, is currently recruiting subjects with OHT and glaucoma (NCT 01033422).
Another class of potential IOP-lowering agents is the selective prostaglandin EP2 receptor agonists.34 One member of this class, taprenepag isopropyl (PF-04217329)35,36 has been evaluated in a phase II clinical trial (n=250).37 Taprenepag 0.0025–0.03% dosed daily produced significantly greater reductions in IOP than placebo (vehicle) and showed similar reductions in IOP compared with latanoprost 0.005% after 14 days in patients with OHT and OAG. In addition, the combination of taprenepag and latanoprost showed significantly greater reductions in IOP than latanoprost 0.005% alone.
Latanoprostene bunod—a novel nitric oxidedonating prostaglandin F2α analog
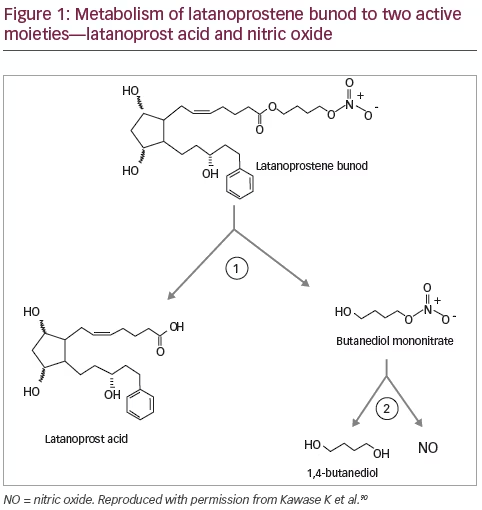
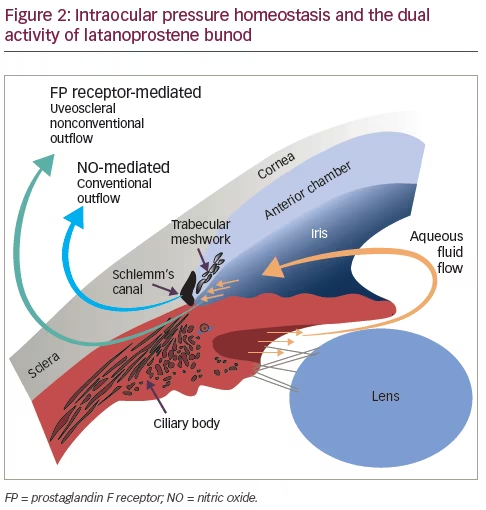
LBN ophthalmic solution 0.024% is an IOP lowering eye drop dosed once daily in the evening for patients with OAG or OHT and is currently under regulatory review by the FDA.38 LBN is a single entity NO-donating prostaglandin F2α analog. Following topical ocular administration, LBN is rapidly metabolized by esterases into latanoprost acid and butanediol mononitrate (BDMN), an NO-donating moiety (Figure 1).39 BDMN is further metabolized to 1,4-butanediol and the signaling molecule, NO. These two active metabolites each have IOP-lowering properties. This factor and various experimental findings have led to the hypothesis that LBN functions via a dual mechanism of action: by increasing both non-conventional (uveoscleral) AH outflow via latanoprost acid and conventional (TM/Schlemm’s canal) AH outflow via NO donation (Figure 2).28,40
The mechanism of IOP reduction by one of the metabolites, latanoprost acid, the active moiety of latanoprost, has been studied extensively. Latanoprost acid lowers IOP by remodeling the extracellular matrix in the ciliary muscle, which increases the uveoscleral AH outflow.41–45,46 Widespread clinical use of the topical PGA latanoprost, an isopropyl ester analog of PGF2α, is based on its ability to lower IOP to a greater extent than other topical agents with a once daily dosing regimen coupled with minimal side effects.28,47–51 The recent United Kingdom Glaucoma Treatment Study was the first randomized, placebocontrolled trial conducted in patients with OAG (n=516) that assessed vision preservation via IOP-lowering in patients treated with latanoprost compared with placebo.52 At 24 months, the mean (standard deviation [SD]) IOP reduction from baseline was greater in the latanoprost group (3.8 [4.0] mmHg) compared with the placebo group (0.9 [3.8] mmHg). In
addition, time-to-first visual field deterioration was significantly longer in the latanoprost group versus placebo group (adjusted hazard risk [HR] 0.44, 95% confidence interval [CI] 0.28–0.69; p=0.0003).
The other LBN active metabolite, NO, is a critical physiologic signaling molecule known for its role as a mediator of smooth muscle relaxation and vasodilation in the body.53–55 NO is produced endogenously from L-arginine by NO synthases and signals via the second messenger cyclic guanosine monophosphate (cGMP).40 In the healthy eye, NO is produced in anterior ocular tissues, including the TM.56,57 Ocular blood flow impairment is hypothesized to contribute to RGC damage58 and several studies have suggested a vasodilatory role of NO on ocular blood vessels,59–61 although no data are currently available to support the potential for RGC rescue or protective properties for LBN. Endogenous NO has been shown to regulate physiological IOP.62 Decreased NO synthase activity in the TM, Schlemm’s canal and ciliary muscle; coupled with decreased NO metabolites levels in the AH of patients with OAG, suggest that reduced NO production likely contributes to the IOP increase.63–65
Outside ophthalmology, nitrovasodilators are used in the treatment and prevention of angina pectoris. In the eye, NO-donating nitrovasodilators have been demonstrated to lower IOP primarily by increasing TM/Schlemm’s canal (conventional) outflow.66 An early clinical study demonstrated that systemic administration of nitroglycerin resulted in IOP lowering in patients with POAG.67 Since then, animal studies have confirmed these nitrovasodilators lower IOP and further demonstrated that this is through an increase in conventional AH outflow.62,68–71 Numerous in vitro and ex vivo studies also suggest that NO-donors relax the tissues of the conventional outflow pathway57,72–75 Ex vivo preparations of bovine and porcine origin also demonstrated the ability of NO donors to reduce AH formation.76,77
Alterations in cell contractility/shape could be the basis of NO-donor mediated IOP-lowering. In vitro studies showed that NO donors
decrease TM cell volume through cGMP signaling and activation of the large-conductance Ca2+-activated K+ (BKCa) channel.57 In addition, NO-donors may induce alterations in the cytoskeletal (actin and myosin) organization of TM and Schlemm’s canal cells via an increase in cGMP.57,73,78,79 NO donors have an inhibitory effect on ROCK, downstream of cGMP in the NO soluble guanylate cyclase (sGC)/cGMP pathway.80,81 ROCK is a serine-threonine kinase that regulates the shape and movement of cells by acting on the cytoskeleton.82 In vascular smooth muscle cells (VSMCs), ROCK mediates the phosphorylation of myosin light chains enabling the contraction of actin fibers.83 TM cells are highly contractile and in this respect, are similar to VSMCs in which NO/sGC/ cGMP signaling activates protein kinase G. Protein kinase G, in turn, promotes relaxation via multiple pathways, including inhibition of ROCK and activation of the large-conductance Ca2+-activated K+ (BKCa) channel. Activation of the sGC/cGMP signaling pathway may therefore result in relaxation in TM cells and Schlemm’s canal, leading to increased aqueous outflow.
Preclinical studies have also demonstrated that LBN has a greater effect on TM cell relaxation than the prostaglandin latanoprost.84 Studies in FP-receptor knockout mice and rabbits, a species which does not respond to latanoprost, have demonstrated that while LBN reduces IOP in these models, there is a lack of effective IOP reduction in response to latanoprost treatment, highlighting the contribution of NO to the IOP lowering efficacy of LBN.39,85 LBN also produced greater IOP lowering than latanoprost in animal models of glaucoma or OHT.39 In ocularly hypertensive primates, LBN achieved a maximum decrease in IOP of 31% and 35% relative to baseline at doses of 0.036% (9 μg) and 0.12% (36 μg), respectively, whereas latanoprost elicited a greater response than vehicle only at 0.1% (30 μg), with a peak effect of 26%. Furthermore, in glaucomatous dogs, IOP decreased from baseline by 44% and 10% following LBN 0.036% and vehicle, respectively, while latanoprost (0.030%) lowered IOP by 27% and vehicle by 9%.39
Clinical studies investigating the use of latanoprostene bunod in glaucoma
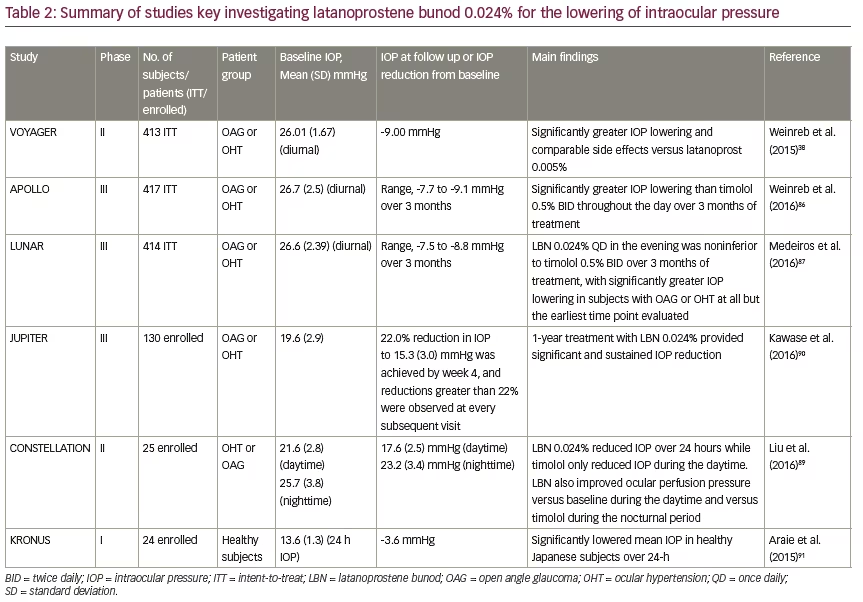
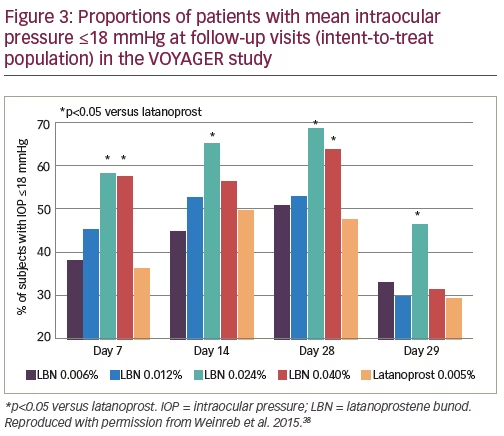
Clinical studies have defined further the activity of LBN in patients with OAG and OHT (Table 2). The VOYAGER study was a phase II, parallel group, dose-ranging study that compared the efficacy and safety of four different concentrations of LBN with latanoprost (0.005%) in patients with OAG or OHT.38 Patients were eligible if they had an IOP of 22–32 mmHg, and an IOP of ≥24 mmHg for at least two of three measurements during Visit 3 (Day 1, baseline), which occurred after a 28-day washout period in subjects previously treated with IOP-lowering medications. Patients were randomized to LBN 0.006% (n=82), LBN 0.012% (n=85), LBN 0.024% (n=83), LBN 0.040% (n=81), or latanoprost 0.005% (n=82) dosed once daily in the evening for 28 days. All doses resulted in significant reductions in mean diurnal IOP from baseline at all follow-up visits (p<0.0001). The response was dose-dependent and plateaued with the 0.024%–0.040% doses. LBN 0.024% was the most effective dose, achieving a greater diurnal IOP reduction compared with latanoprost 0.005% at Day 28 (p=0.005). The difference in reduction of diurnal IOP between LBN 0.024% and latanoprost 0.005% at Day 28 was 1.23 mmHg. On secondary efficacy assessments, there were significantly greater reductions in mean diurnal IOP versus latanoprost at day 7 for the LBN 0.024% and 0.040% groups (p=0.033 and 0.009, respectively), and at Day 14 for the LBN 0.024% group (p=0.015). Significantly greater reductions in mean IOP were also observed for LBN 0.024% compared with latanoprost 0.005% at most individual time points. In addition, a significantly greater proportion of subjects had mean diurnal IOP ≤18 mmHg in the LBN 0.024% group at day 28 compared with the latanoprost 0.005% group (Figure 3). LBN was well tolerated but instillation site pain appeared to occur more frequently with LBN 0.024% (12%) versus latanoprost 0.005% (6.1%).
The clinical development program of LBN has continued with two recent phase III, randomized, double-masked, parallel-group clinical studies (APOLLO and LUNAR). The APOLLO study (n=420) was a randomized, controlled, multi-center, double-masked, parallel-group clinical study that compared the 3-month efficacy (IOP reduction) and safety of LBN 0.024% with that of timolol maleate 0.5% (randomized 2:1, respectively) in patients with OAG or OHT in one or both eyes (IOP range: 22–36 mmHg).86 Eligible patients had an IOP ≥26 mmHg at a minimum of 1 time point, ≥24 mmHg at a minimum of one time-point, and ≥22 mmHg at one time-point in the same eye, and IOP ≤36 mmHg at all three time-points in both eyes at baseline. Eligible patients received topical doses of LBN 0.024% QD (evening) or timolol 0.5% BID (morning and evening) for 3 months and IOP measurements were made at baseline (at 8 am, 12 pm and 4 pm), and at 8 am, 12 pm and 4 pm during study visits at 2 weeks, 6 weeks and 3 months (nine time points) after the start of treatment.
Mean IOP in the study eye in the intent-to-treat population, which was the primary endpoint, was significantly lower in the LBN 0.024% group (range, 17.8–18.7 mmHg) than the timolol 0.5% group (range,19.1–19.8 mmHg) at all 9 time points (p≤0.002 for all), confirming not only non-inferiority to timolol
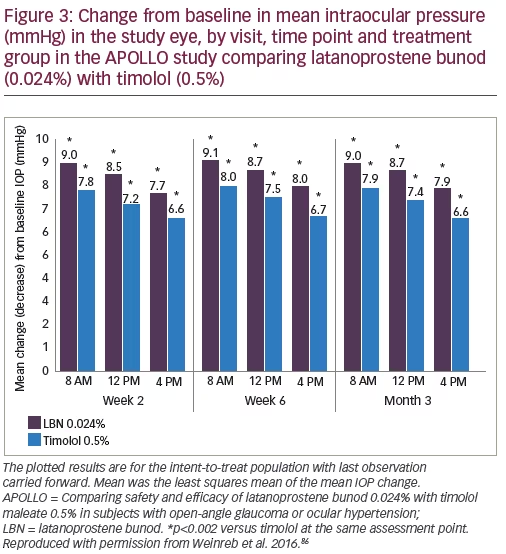
but significantly greater IOP-lowering to timolol.86 The change in mean IOP from baseline was also significantly greater for LBN 0.024% compared with timolol 0.05% at all 9 time points (p≤0.002 for all) (Figure 4).
For secondary endpoints, at all nine time points, the proportion of subjects with mean IOP ≤18 mmHg was significantly greater with LBN 0.024% versus timolol 0.5% (mean IOP ≤18 mmHg: 22.9% versus 11.3%, p=0.005).86 The percentage of subjects with IOP change from baseline ≥25% was also significantly greater for LBN 0.024% than timolol 0.05% (34.9% versus 19.5%, p<0.001). A further ANCOVA analysis showed that the mean change from baseline in IOP for LBN 0.024% (range, –7.7 to –9.1 mmHg) was significantly greater than that of timolol 0.5% (range, –6.6 to –8.0) for all nine time points (p≤0.002).86
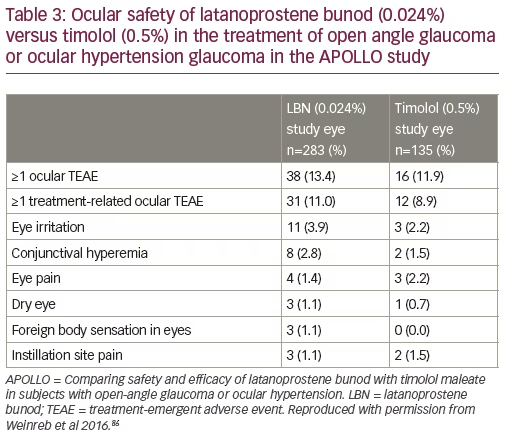
The occurrence and types of ocular adverse events in the APOLLO study were similar in both treatment groups (Table 3).86 Treatment-emergent adverse events (TEAEs) occurred in 13.4% of LBN 0.024% and 11.9% of timolol 0.5%-treated patients. The most frequent events were eye irritation, conjunctival hyperemia, and eye pain. Two patients in the LBN 0.024% group and five in the timolol 0.5% group discontinued due to ocular adverse events. Similar proportions of patients receiving LBN 0.024% or timolol 0.5% had non-ocular TEAEs (12.7% and 14.1%, respectively). The proportions of patients with these TEAEs that were considered treatment-related were 1.8% and 2.2%, respectively. It was concluded that LBN 0.024% was safe and significantly more effective than timolol 0.5% for IOP lowering. In addition, the ability to reduce IOP ≤18 mmHg with LBN may be a significant advantage over topical β-blockers.
The findings of the similarly designed LUNAR study (n=420) indicate comparable IOP lowering to the APOLLO study between LBN 0.024% and timolol 0.5% over 3 months.87 At all but one of the measured time-points (i.e. 12 pm, 4 pm, at week 2, 8 am, 12 pm and 4 pm at week 6 and month 3), the mean IOP in the study eye was significantly lower in the LBN 0.024% group than in the timolol 0.5% group. Results from APOLLO and LUNAR showed that LBN 0.024% reduced mean IOP values by 7.5 to 9.1 mmHg over the three months’ treatment. Following completion of the double-masked efficacy phase, all patients were switched to open-label treatment with
LBN 0.024% once daily in the evening for another 9 (APOLLO) or 3 (LUNAR) months. From pooled data from the APOLLO and LUNAR open-label safety extension phase (number of patients completed the studies=737), subjects randomized to timolol who were switched to LBN in the safety extension phase demonstrated an additional 6.3–8.3% decrease in mean diurnal IOP; IOP lowering was sustained over the entire duration of the studies.88 Overall, 18.7% of subjects who received LBN experienced ocular TEAEs (study eye); the most common of these were conjunctival hyperemia (5.9%), eye irritation (4.6%), eye pain (3.5%). The majority (>99.5%) of ocular TEAEs were mild-moderate in severity. There were no safety issues with regard to ocular signs, best corrected visual acuity (BCVA), and vital signs, or endothelial cell stress with LBN based on specular microscopy.
Treatment with LBN 0.024% once daily resulted in IOP lowering during both the diurnal/wake and the nocturnal/sleep period in the CONSTELLATION study.89 In this prospective, open-label randomized crossover trial in 25 patients with OHT or OAG, LBN 0.024% treatment was associated with a reduction in both diurnal and nocturnal IOP versus baseline whereas timolol 0.5% reduced IOP only during the diurnal period.89 In addition, LBN 0.024% treatment resulted in a significant increased diurnal ocular perfusion pressure versus baseline and nocturnal ocular perfusion pressure versus timolol 0.05%.
In the single-arm, multicenter, open-label JUPITER study, the long-term safety and efficacy of LBN 0.024% was studied over 1 year in 130 Japanese subjects with OAG and OHT with a mean (SD) baseline IOP of 19.6 (2.9) mmHg.90 At 52 weeks, the mean reduction in IOP was 5.3 mmHg or greater than 25% from baseline in the study eye. Long-term treatment in this study provided significant IOP reduction that was sustained up to a year. Finally, LBN 0.024% dosed QD for 14 days, was showed to significantly lower mean IOP during a 24-hr period in 24 healthy Japanese subjects in the singlecenter, open-label KRONUS study91 with a mean (SD) 24-hour reduction of 3.6 (0.8) mmHg or 27% from the baseline in the study eye.91 Mean (SD) baseline IOP was 13.6 (1.3) mmHg in the study eye.91 Peak and trough IOP lowering occurred at 8 AM and 8 PM (i.e. 12 and 24 hours following instillation) with a mean reduction of 4.2 (1.8) mmHg, or 30%, and 2.8 (2.2) mmHg, or 20%, respectively.
Collectively, the VOYAGER, APOLLO, LUNAR, CONSTELLATION, JUPITER, and KRONUS study findings are likely to make a robust case for the use of topical LBN 0.024% in OAG and OHT. Further, data from the JUPITER and KRONUS studies suggest that LBN may by effective in lowering IOP in patients with NTG.
Summary and concluding remarks
While effective, many of the current topical medical treatments are limited by systemic or local side effects, multiple instillations per day, and lack of 24-hour control of IOP. LBN is hypothesized to increase AH outflow by targeting both the uveoscleral (via latanoprost acid) and TM (via NO) pathways and is under regulatory review by the US FDA as a once-daily single-agent topical medication for IOP lowering in patients with OAG or OHT. Evidence from phase II and phase III clinical studies demonstrated that once-daily LBN lowers IOP in patients with OAG or OHT to a greater extent than latanoprost 0.005% and timolol 0.5%.38,87,86 The observed 1.23 mmHg difference in mean diurnal IOP change from baseline between LBN 0.024% and latanoprost 0.005% in the phase II trial was statistically significant and may be considered clinically significant in reducing the risk for progression of glaucoma. These findings are supported and greatly extended by the results of the larger phase III APOLLO study in which IOP was significantly lower with LBN 0.024% treatment than timolol 0.5% at all time points over 3 months. Results from the second phase III (LUNAR) study are consistent with these findings. LBN appears to have a dual mechanism of action in lowering IOP and has demonstrated the potential to provide sustained 24-hour IOP reduction in healthy subjects and patients with elevated IOP.89,91 Obtaining superior effects from fewer doses of medication could make a difference in both patient adherence and compliance. Long-term (1 year) data on LBN’s sustained IOP lowering efficacy has recently been published90 and further investigation is required to explore the additional beneficial properties and safety with long-term use of LBN and specifically in subjects with NTG.
The addition of LBN QD single-molecule monotherapy that targets both outflow pathways to the glaucoma treatment armamentarium offers the potential of increased IOP lowering efficacy without sacrificing safety when compared with currently available topical glaucoma therapies.
APOLLO = Latanoprostene Bunod 0.024% versus Timolol Maleate 0.5% in Subjects with Open-Angle Glaucoma or Ocular Hypertension: The APOLLO Study CONSTELLATION = Efficacy of Latanoprostene Bunod Compared with Timolol 0.5% in Lowering IOP over 24 h JUPITER = Long-term Safety and Efficacy of Latanoprostene Bunod 0.024% in Japanese Subjects with Open-Angle Glaucoma or Ocular Hypertension: The JUPITER Study KRONUS = Evaluation of the Effect of Latanoprostene Bunod Ophthalmic Solution, 0.024% in Lowering Intraocular Pressure over 24 h in Healthy Japanese Subjects LUNAR = Comparison of Latanoprostene Bunod 0.024% and Timolol Maleate 0.5% in Open-Angle Glaucoma or Ocular Hypertension: LUNAR VOYAGER = A Randomised, Controlled Comparison of Latanoprostene Bunod and Latanoprost 0.005% in the Treatment of Ocular Hypertension and Open Angle Glaucoma: the VOYAGER Study


