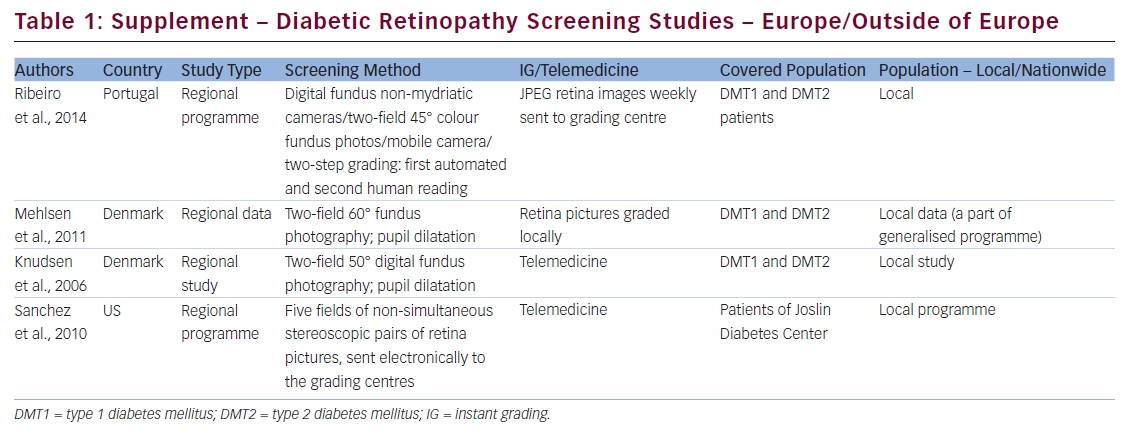
We recently published a review of diabetic retinopathy (DR) screening methods and programmes adopted in different parts of the world.1 After publication we learnt about more DR screening programmes and believed that this important information should be supplemented with data from Portugal, Denmark and the US (see Table 1).
Portugal
Ribeiro et al.2 presented a study on DR screening based on non-mydriatic fundus images augmented by automated disease/no disease grading. The screening programme has been performed in the Central Region of Portugal since 2001. They improved their screening by implementation of automated grading software, Retmarker screening technology, in 2011. They use mobile fundus cameras and a photographer/screener for each geographic area. The photographer/screener prepares weekly reports and sets of JPEG retina images and sends them to the grading centre. The automated, two-step grading analysis of retina pictures reduces the burden of reading centres and improves the sensitivity and specificity of DR detection.3 The grading process consists of two steps: (1) automated analysis and (2) human grading. Humans grade only pictures classified as suspected of having DR and pictures with poor quality. This procedure reduces the amount of fundus pictures required to be seen by humans.
Denmark
There is a national DR screening programme in Denmark, but there are no generalised English-language publications on it. All data are available on its Danish website.4 We can find some information about the programme from selected regional studies. Mehlsen et al.5 described a study based on the database for DR at the Department of Ophthalmology, Aarhus University Hospital. Their DR screening is based on fundus pictures, which are graded by a certified nurse grader and in problematic cases of retina by specialists. The same authors6 suggest that it is possible to customise DR screening intervals by construction of a model optimising DR intervals for low-risk DR patients. Knudsen et al. described another regional Danish DR screening study.7 They presented the North Jutland DR study based on digital-colour retina pictures and subsequent remote grading.
The US
Sanchez et al.8 described a telemedicine system of Joslin Vision Network developed in the Beetham Eye Institute, Boston, Massachusetts. It is based on digital five fields of non-simultaneous stereoscopic fundus photographs taken by non-mydriatic retinal cameras, and the photographs are digitally sent to the grading centre. The status of eye fundus and recommendations are sent to the patients. This system has been adopted in several US vision centres. The new retinal imaging with ultrawide fundus pictures compared with non-mydriatic fundus imaging seems to be more efficient in DR detection.9 Silva et al.10 suggest that ultrawide field retinal imaging graded by trained non-physicians has a good sensitivity and specificity for detection of DR. They concluded that immediate evaluation of pictures reduces grading-centre burden by 60 % and patients’ feedback should be expedited.
Rectification
We would like to correct the data in Table 1 in our recently published article titled ‘Review of Diabetic Retinopathy Screening Methods and Programmes Adopted in Different Parts of the World’.1 The data for Diabetic Retinopathy Screening Service for Wales in the column ‘Instant Grading/Telemedicine’ should be ‘Telemedicine’.