




The health of the corneal endothelium, the innermost single cell layer of the cornea, is essential in maintaining corneal transparency. This is achieved through a passive diffusion of fluid across leaky inter-cellular tight junctions from the aqueous humor into the corneal stroma and active ionic pumps, which moves fluid against an osmotic gradient from the corneal stroma back into the aqueous humour.1–4 This “pump-leak” mechanism maintains the corneal aqueous content at an ideal level of 78%. This supports optimal inter-lamellar spacing of collagen fibrils within the corneal stroma to achieve corneal transparency.5,6
An accelerated loss of corneal endothelial cells occurs in diseases of the corneal endothelium, such as Fuchs’ endothelial corneal dystrophy or ocular insults including intraocular surgeries, anterior segment laser treatments, ocular trauma or inflammation. When the corneal endothelial cell density falls below a certain threshold, the ability of the corneal endothelium to regulate corneal hydration becomes impaired.7–9 In corneal endothelial failure, the cornea becomes edematous, resulting in a loss in its transparency and eventual visual impairment.
Visual impairment from corneal endothelial failure is a leading indication for corneal transplantation.10,11 Over the past two decades, there has been a fundamental shift in the treatment of corneal diseases towards replacing only diseased parts of the cornea.12,13 Indeed, the concept of selective replacement of damaged endothelial cells has revolutionized the treatment of corneal endothelial failure.13 Such corneal transplantation techniques, known as endothelial keratoplasties (EKs), are able to achieve improved visual outcomes, lower risks of graft rejection, and superior graft survival rates, compared to traditional full-thickness penetrating keratoplasties (PKs).14,15 As these EK techniques are minimally invasive, they avoid full-thickness central corneal trephination and intraoperative ‘open-sky’ situations, thereby reducing the risk of sight-threatening complications like expulsive hemorrhage. They also offer better mechanical integrity and overall globe strength. EKs have thus replaced PKs as the standard of care for treating corneal endothelial failure.10,11,16
In current clinical practice, there are two leading EK techniques: Descemet’s stripping automated endothelial keratoplasty (DSAEK) and Descemet’s membrane endothelial keratoplasty (DMEK). In DSAEK, transplanted donor endothelial grafts consist of donor endothelium, Descemet’s membrane, and some posterior stroma. Since its introduction, much research has been focused on methods to improve the post-operative outcomes of DSAEK surgical technique. Advancements such as the development of devices for graft insertion have greatly simplified DSAEK.17 These devices include the Busin Spatula (Moria Ophthalmic Instruments, Antony, France),18 the DMEK EndoGlide™ (Network Medical Products, Rippon, UK),19 and the EndoSaver® (Ocular Systems Inc, Winston Salem, NC, USA), amongst various others. Such devices maintain graft orientation during graft insertion and are less traumatic to the endothelium as they minimize the need for intraocular manipulation when unfolding the graft.17 With predictable visual outcomes and improved graft survival compared to PK, DSAEK has been widely adopted by corneal surgeons.11
DMEK is the more recent advancement in EK surgery. In DMEK, only the Descemet’s membrane with its endothelium is harvested from donor tissue and is transferred into the recipient’s eye. By only replacing tissues affected by endothelial diseases, DMEK is anatomically more accurate. Indeed, DMEK has been shown to achieve more rapid visual recovery and better visual outcomes compared to DSAEK.20–23 Unlike DSAEK, as stromal tissue is not transplanted in DMEK, a change in corneal profile is avoided in the latter. DMEK is thus associated with improved refractive outcomes.21 Recent studies comparing DMEK and DSAEK have also reported lower endothelial rejection rates in DMEK.24
Despite the advantages of DMEK over DSAEK, many corneal surgeons have been slow to adopt DMEK as the main procedure to treat endothelial failure.12 According to the Eye Bank Association of America (2018 Eye Banking Statistical Report—page 6), DSAEK still accounts for over 60% of EK procedures performed in the United States.11 This has been attributed to the challenges in surgical techniques and the associated increased early post-operative complications, notably graft detachments and iatrogenic graft failures due to inadvertent ‘inverted ’ grafts.
Endothelium-out DMEK techniques
Current techniques of transferring the DMEK graft into the anterior chamber involve the insertion of the graft through a small corneal incision. In ‘endothelium-out’ techniques, the DMEK graft is loaded and inserted such that its endothelium remains on its outer surface (Figure 1). The first DMEK, introduced by Melles, was an endothelium-out technique,25 and there have been various modifications to this technique since. Thus, the vast majority of techniques used in published studies are endothelium-out techniques.22,26–37
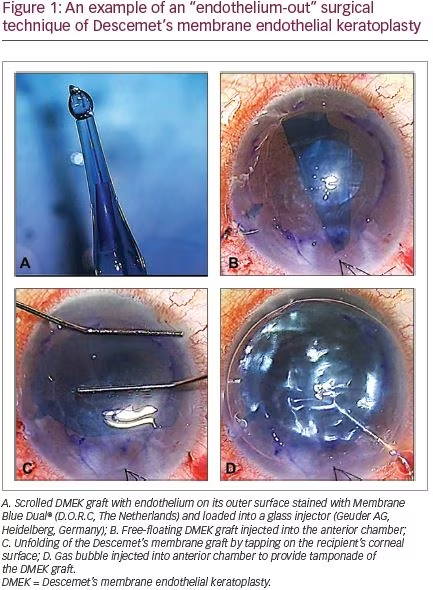
To protect the Descemet’s membrane scroll from the surgical wound, different instruments have been designed for DMEK graft insertion. These include glass injectors38,39 and intraocular lens cartridges.40,41 Nevertheless, being endothelium-out, the DMEK graft is still potentially susceptible to endothelial cell loss caused by contact of its endothelium with the lumen of the insertion device. Furthermore, endothelium-out techniques all involve the injection of the scroll of DMEK graft into the anterior chamber in its entirety, leaving the surgeon to unscroll the free-floating graft within the eye.
The unscrolling of a free-floating DMEK graft, after its intraocular insertion, is considered the most difficult step in DMEK. It can be challenging, unpredictable, and time consuming.42 The challenge comes from the fact that the Descemet’s membrane, once separated from the stroma, has a natural tendency to form a scroll with its endothelium on its outer surface. The scroll can be tight, especially for tissues harvested from younger donors. Compared to DSAEK, different surgical skills with steeper learning curve are required by the surgeon.43 The surgeon must learn various techniques to unfold a free-floating DMEK graft within the anterior chamber (Figure 1).44–46 Such techniques include methodological approaches to unfolding a double-scrolled graft by tapping the cornea in a shallow anterior chamber, the use of intracameral water currents to shift and orientate the graft and air bubbles to assist in tight or single scrolls.45,46 As endothelium-out techniques are reliant on such water currents and air bubbles in graft unscrolling, surgery can be difficult in eyes with abnormal anterior segments (e.g., iris defects). In cases such as tight graft scrolls or a very deep anterior chamber, the unfolding of the graft can also be technically challenging.47
Endothelium-in DMEK techniques
The concept of “endothelium-in” graft insertion techniques for DMEK surgery has recently been introduced (Figure 2).48–51 After harvesting, the DMEK graft is folded, often in a tri-fold, with its endothelium on its inner surface. This prevents the graft from naturally scrolling with its endothelium on the outer surface. Such endothelium-in techniques are thought to have the advantage of minimizing endothelial cell loss from trauma of the endothelial cells on the luminal walls of insertion devices. Furthermore, in endothelium-in techniques, the donor tissue is inserted into the eye in the correct orientation with the endothelium facing downwards. Following insertion in an endothelium-in configuration, the DMEK graft starts to unfold to adopt its natural endothelium-out scroll, essentially “assisting” the surgeon in graft unfolding. Moreover, endothelium-out techniques use water currents and air bubbles in the anterior chamber to orientate and unscroll the free-floating graft and thus surgical complexity is dependent on anterior segment anatomy. Such reliance on a normal anterior segment (e.g., intact iris diaphragm) is circumvented in endothelium-in techniques. These features of endothelium-in techniques thus minimize the surgical challenges of graft orientation and unfolding of a free-floating scrolled graft within the eye, making surgery more controlled and predictable.
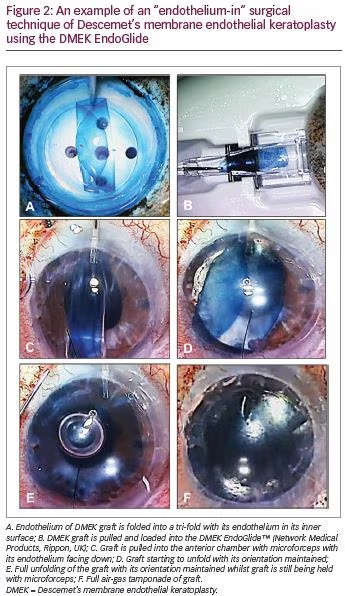
Endothelium-in techniques can be inserted into the eyes by a) direct injection into the anterior chamber or b) pulled into the eye using various pull-through devices or intraocular lens cartridges. In eyes with normal anatomies, endothelium-in techniques provide unfolding advantages as described above, whether the graft is injected or pulled into the eye. In eyes with abnormal anatomies (e.g., iris defects, previous vitrectomies, aphakia), pull-through methods have tremendous advantages. Furthermore, various pull-through devices have been designed to mimic DSAEK procedures, which are familiar to many corneal surgeons.48
Outcomes of endothelium-out and endothelium-in techniques
Endothelium-out techniques
In current literature, the vast majority of published studies on DMEK are based on endothelium-out techniques.22,26–37,52 Studies published are mainly retrospective case control studies or case series.52 At 6 months, 42.5–75.0% of cases have been reported to achieve a best-corrected visual acuity (BCVA) of 20/25 or better, and 17–44% have been reported achieve a BCVA of 20/20 or better.52 Mean endothelial cell losses have ranged from 19–53% amongst various studies with a mean time point of 12 months.52 For graft complications, re-bubbling rates, primary graft failure rates, secondary graft failure rates, and graft rejection rates ranged from 0.0–82.0%, 0.0–18.2%, 0.0–7.0%, and 0.0–7.0% respectively.52
Endothelium-in techniques
We found only three studies in the literature that used endothelium-in techniques, all of which were retrospective studies.48–50,52 In one study, 66.7% of cases achieved BCVA of 20/25 or better at 3 months.48 The mean endothelial cell loss ranged from 29.5–56.0% (two studies) with a mean time point of 12 months.48,49 Reporting on complications, graft detachment re-bubbling rates and primary graft failure rates ranged from 10.0–34.1% (three studies)48–50 and 0.0–3.0% (two studies),48,49 respectively.
One recent case control study of 754 cases compared endothelium-out to endothelium-in DMEK graft insertion techniques.51 No significant differences in endothelial cell loss, rates of re-bubbling for graft detachments, and primary graft failure rates were found between the two techniques. Various laboratory studies have reported no significant differences in endothelial cell loss when DMEK grafts were loaded endothelium-in and pulled-through or loaded endothelium-out and injected-through different graft insertion devices.53–55 However, pre-clinical laboratory studies have also reported significantly shorter graft unfolding times for endothelium-in compared to endothelium-out techniques.55
Conclusion
Despite the small number of studies reporting on endothelium-in techniques, current evidence suggests that the outcomes of these techniques are comparable to outcomes of endothelium-out techniques. With the intra-operative challenges of unscrolling a free-floating DMEK graft encountered in endothelium-out techniques, corneal surgeons may wish to consider adopting endothelium-in DMEK techniques. This is especially the case in more challenging eyes with complex anterior segments (e.g., aphakia, large iris defects, vitrectomized eyes, previous glaucoma filtration surgery), where many surgeons still prefer DSAEK in these situations.


