




Few, if any studies are available on the prevalence and spectrum of ocular chlamydial disease in the US. Current estimates of ocular disease are predominantly anecdotal. The majority of disease is associated with urogenital transmission, with conservative estimated rates of one case for every 300 genital cases. According to Kalayoglu, 50–90% of adults with ocular chlamydia have concomitant genital disease.1 Two thirds of neonates born to infected mothers will become colonized and one third of these will develop clinical evidence of neonatal inclusion conjunctivitis.
The true prevalence and public health burden, however, is unknown. None of the US sexually transmitted disease (STD) screening programs or clinics screen for ocular chlamydia. Nor do ophthalmologists and other ophthalmic healthcare providers routinely ask or screen for genital or extragenital infections.
The chlamydiae are non-mobile, gram negative, obligate, intracellular, energy parasites recovered from a variety of hosts, systemic, and ocular infections. Chlamydial species possess a unique and complex multiphasic developmental cycle, which requires living tissue for cultivation and growth.
A variety of ocular diseases are associated with chlamydia and chlamydia-like microorganisms worldwide. The order, Chlamydiales includes nine families, Chlamydiaceae, Clavichlamydiaceae, Criblamydiaceae, Piscicchlamydiacea, Parachlamydiaceae, Rhadochlamydiaceae, Simkaniaceae, Wadddliaceae and ‘Candidatus’ Parilichlamydiae more than 20 species.2 Currently, only members of two families (Chlamydiaceae and Parachlamydiaceae) and five species (C. trachomatis, C. pneumoniae, C. psittaci, Neochlamydia and Parachlamydia) have been associated with ocular infections.3–10
C. trachomatis causes the majority of ocular disease, including trachoma,2 neonatal and adult inclusion conjunctivitis,11,12 keratitis,1,13 uveitis,14 and lymphoma.15
C. pneumoniae is a major respiratory pathogen. Seroprevalence ranges from 40–80%. Reports of ocular disease is rare. It has been recovered in patients in endemic trachoma area,16 patients with follicular conjunctivitis,17 and adults with keratoconjunctivitis.17
C. psittaci is endemic in pet and wild birds including parrots, pigeons, and parakeets. It causes psittacosis and or orthniosis, a systemic disease involving the conjunctiva. C. psittaci has been detected in endemic trachoma areas16 and in ocular adnexa lymphomas (OALs) tissues in patients from Italy and Asia.14,18,19
Family Parachlamydiaceae and family Rhadodochlamydiaceae
These emerging chlamydial-like organisms are endosymbionts of free living amoeba (Acanthamoeba and or Hartmartnella) species.3,6,20 They can cause respiratory and ocular disease in humans.3,6,20 The spectrum of chlamydia species in ocular chlamydia is unknown.
Similar to genital disease, the diagnosis and detection of chlamydial species in ocular tissues can be difficult.21,22 Signs and symptoms often mimic other bacterial, viral infections, or allergic conjunctivitis. Chlamydia infections may present with only minor clinical signs and pose a significant therapeutic predicament for the ophthalmologist.12,23
Complications following ocular chlamydia infections are varied. They may include and result in life-long and life-threatening sequelae, including chronic disease, corneal scarring, uveitis, asthma, and obstructive lung disease.1,23,24
Methodology
This was a laboratory-based surveillance to document prevalence and compare the diagnostic efficacy of three nonculture or antigen detection methods, direct fluorescent antibody (DFA), enzyme immunoassay (EIA), and nucleic acid amplification techniques (NAAT) relative to tissue culture to confirm the presence of chlamydia antigens in ocular tissue. Historical and current use data were collected from laboratory reports and entered into a SPSS database for comparison of performance characteristics and trends for two time periods (historical; 1986–2004, 18 years) and more recent (2005–2014, 10 years). Frequency and age specific rates were calculated per method and annually.
Statistics Test comparisons were calculated for samples in which two or more diagnostic evaluations were performed. Prevalence data and cross tabulations on age and sex were evaluated using 2 x 2 chi square tables. McNemar’s matched pair test Z tests and or tests of proportions were used to determine significance and test performance characteristics (sensitivity, specificity, positive and negative predictive values). Data analysis was also supplemented using Excel.
Patient population
The patient population consisted of 3,112 consecutive patients (1,640 women and 1,472 men) evaluated at the Bascom Palmer Eye Institute Microbiology Laboratory to rule out ocular chlamydia from January 1986 to December 2014. Age ranged from 2 days to 98 years.
Specimens
Scrapings from ocular tissues, greater than 90% from the conjunctiva were collected with Dacron swabs or a platinum spatula after removable of obvious purulent discharge and placed within an inscribed circle on a glass slide for DFA. A second swab was collected and placed in chlamydia, EIA, polymerase chain reaction (PCR), or ligase chain reaction (LCR) transport media (2 ml) for culture, EIA, and/or nucleic acid amplification tests. Tissue biopsies from cornea or lids were placed in balanced salt solution in a sterile petri dish, sent to the microbiology laboratory for processing. Samples were collected and processed in accordance with manufacturer’s instructions.
Direct fluorescent antibody
Scrapings were placed inside the well of the slide provided in the Micro- Trak® (Syva Inc, Palo Alto, CA, US). DFA kit and appropriately labeled with patient’s name, source, and date of collection. Patient positive and negative control slides were fixed in acetone for 10 minutes. One drop (approximately 30 ul) of monoclonal antibody directed against the major outer membrane protein (MOMP) of chlamydia was added to each patient and or control well. Slides were incubated for 15 minutes at room temperature in a moist chamber. Slides were rinsed with sterile phosphate buffer for 10–15 seconds and air-dried. One drop of mounting fluid included in the kit was added to each patient and/or control well. The slides were screened with an epifluorescence microscope at a total magnification of 400x without oil. Positive slides were confirmed using a 100x oil immersion objective. Slides with less than five epithelial cell per high power field were rejected as inadequate. A positive result was scored as the presence of 10 or more apple green fluorescent round to oval elementary bodies (300 ul).
Enzyme immunoassay
Two-enzyme immunoassays were used to detect chlamydia in ocular tissue. The first of these, the Bartels PRIMA (Bartels [Intracel] Inc., Seattle, Washington) was a manual microwell system for detection of chlamydia antigen. Scrapings were collected and placed in the Bartels EIA transport medium or aliquots from cryopreserved or general chlamydia transport media (Bartels, Bartels, Seattle Washington) were processed according to manufacturer’s suggestions. The VIDAS chlamydia (BioMerieux, St. Louis, MO, US) is an enzyme-linked fluorescent immunoassay. All assay steps are performed and controlled by the instrument, but the principle is the same as the Bartel’s PRIMA system. Scrapings were collected as above and placed into the VIDAS transport media. Samples were treated and processed in accordance with the manufacturer’s instructions.
Polymerase chain reaction
The protocol for the detection of chlamydia by the polymerase chain reaction (PCR) was a manual protocol, designed in the laboratory in accordance with specifications of Bobo et al.25 The 24 base pair primers (oligonucleotides) for the PCR (5’-A/CGT/TCG/CAG/GAA/GCC-3’, 5’-AAC/TCA/AAA/CCC/TCT/CAT/TCT/ CAA-3’) for the amplification of C. trachomatis were obtained from Genemed Biotechnologies, Inc (South San Francisco, CA, US). Thermocyclers used for the amplification of the product were purchased from the Perkin Elmer Corporation (Norwalk, CT, US) or Gene Machine (Atlanta, GA, US).
The reaction mixture was first heated to 94 ºC for 1 minute, cooled to 55 ºC for 1 minute, followed by raising the temperature to 72 ºC and incubating for 1 minute to extend the DNA chain. This procedure was repeated for a total of 32 cycles. A final 10-minute incubation at 72 ºC was carried out for the ending cycle. A 2% agarose gel containing 0.5 μg/ml ethidium bromide was prepared, 10–20 μl of the amplified samples and or controls applied and subjected to electrophoresis for 2–4 hours. Detection of a band containing a 182 base pair product, with appropriate bands for positive and kit controls, complimented with no band for the negative control was scored as a positive result.
Ligase chain reaction
The Abbott LCX LCR (Abbott Laboratories, Abbott Park, IL, US) is an automated procedure which employs oligonucleotide pairs to target gene sequences in the cryptic plasmid found in multiple copies in C. trachomatis or gene sequence in Neisseria gonorrhoeae. All tests were performed in accordance with the manufacturer’ specifications. Swabs with scrapings from conjunctiva and cornea or aliquots from cryopreserved samples were heated to 97ºC for 15 minutes and cooled, specimens were expressed from the swabs and the swabs discarded. One hundred microliters of the remaining fluid was added to a 100 μl tube LCR mixture. Amplification was carried out for 40 cycles for 1 second at 93 ºC, 1 second at 59 ºC and 1 minute 10 seconds at 62 ºC. One hundred microliters of the amplified product was transferred to a reaction cell, which was placed in the analyzer for detection of chlamydia or N. gonorrhoeae.
Culture
Ocular samples for culture were received in chlamydia transport media, vortexed and 0.1 ml of media inoculated into one light density and one moderate density cycloheximide-treated McCoy cells on glass coverslips in shell vials. Vials were incubated at 37 ºC for 48–96 hours and stained for chlamydia at 48 and 96 hours using the Sylva Monoclonal antibody kit (Sylva, San Jose, CA, US) Specimens with greater than one inclusion or reticulate body were considered positive.
A Multiplex PCR using Qiagen Hot Start technique and species specific primers for C. pneumoniae and C. trachomatis were used to screen random samples collected between 1994 and 2014 to document the presence of nontrachomatis species and or mixed species among this group. Primers sequences included:
• Cpn 90 Madico F 5’ GGTCTCAACCCCATCCGTGTCGG 3’;
• Cpn 91 Madico R 5’ TGCGGAAAGCTGTATTTCTACAGTT 3’;
• Ctr70 trachomatis F 5’ GGCGTATTTGGGCATCCGAGTAACG 3’; and
• Ctr71 trachomatis R 5’ TCAAATCCAGCGGGTATTAACCGCCT 3’.
The cycling parameters: one cycle at 95 oC for 15 minutes, followed by 35 cycles with a denaturation step at 94 oC for 30 seconds, an annealing step at 62 oC for 30 seconds, and an extension step at 72 oC for 30 seconds, followed by one cycle of extension at 72 oC for 9 minutes. Amplified products were detected by electrophoresis.
Gold standard
Nonculture tests (DFA, Bartels-EIA, VIDAS-EIA, PCR and LCx) were compared with the ‘gold’ standard of a positive culture and an ‘expanded gold standard’ of positive culture and/or two positive nonculture tests. CDC defines positivity rates for chlamydia as the number of positive tests divided by the number of adequate tests performed.
Results
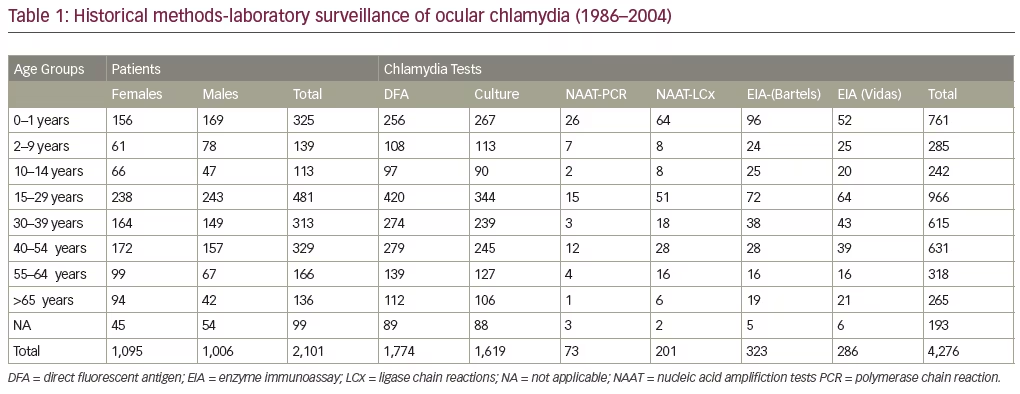
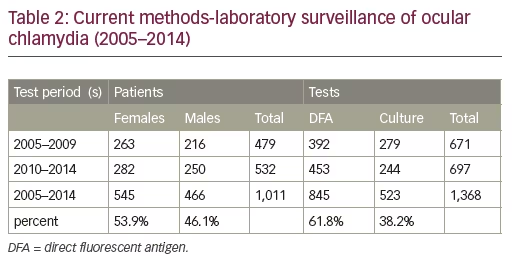
A total of 3,112 patients and 5,644 tests were evaluated over the 28-year period. The ages ranged from two weeks to 98 years, with females constituting 52.7% (n=1,640) versus 47.3% (n=1,472) for males (see Tables 1 and 2).
Chlamydia antigens were documents in all age groups and both sexes by multiple test methods. Trends in historical and recent positivity chlamydia rates are displayed in Figure 1.
Chlamydia positive rates ranged from 5.8% to 13.4% with a median prevalence rate of 10.5%. Overall prevalence (positivity) rates for ocular chlamydia steadily declined from the earliest test period, 1986–1989 (13.4%) by twofold to 5.8% (p=0.00014) for the last fiveyear test period (2010–2014). The culture positive rate was almost three times (2.7x) as high during the historical period 1986–2004, 8.5% (n=137/1619) compared to the last 10 years, 3.1% (n=523), 3.9% for test
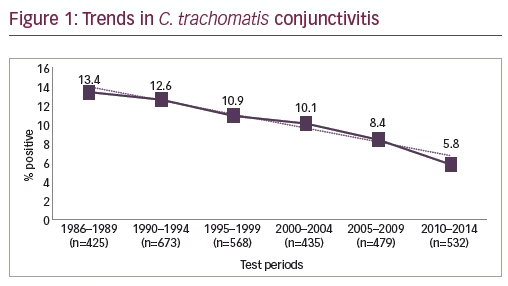
period 2005–2009 (n=11/279) and 2.0% for the most recent test period 2010–2014 (n=5/244).
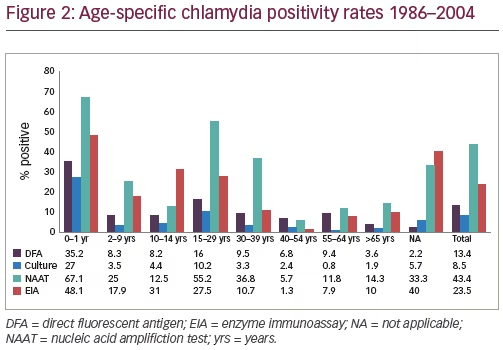
Figure 2 displays the historical age specific rate by test method. Age specific detection or positivity rates for chlamydia varied by tests methods. The highest rate of chlamydia was documented in age group 0–12 months for all tests and ranged from 27.3% (culture) to 73.9% (PCR). The second highest rate in five of the six tests was for age group 15–29 years (10.2%-culture to 58.6%-LCR). No significant differences between rates for age groups for culture (8.6%) or the expanded gold standard (10.3%). Age specific rates were also highest in males (12/120, 10%, 24.5%) and age group 15–29 (10/41, 24.5%) for data collected for the last 30 months of period II (2005–2014).
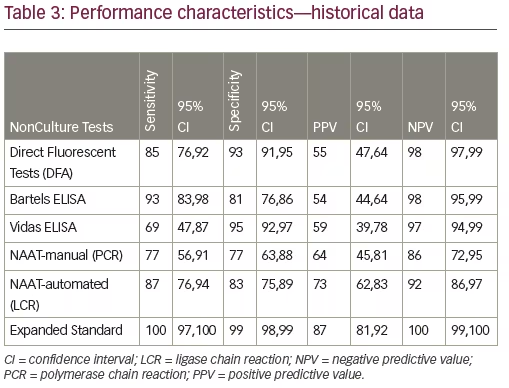
Performance characteristics (sensitivity, specificity, PPV, and NPV) for the culture independent chlamydial tests versus culture as the gold standard of tissue culture are displayed in Table 3. The laboratory test with the highest values for the combination of sensitivity and negative predictive value to ‘rule out’ chlamydia relative to culture was Bartels EIA (93% and 98%, respectively). In descending order, results for the remaining tests were: DFA (85% and 98%), LCR (87% and 92%), PCR (77% and 86%), and VIDAS (69% and 97%). Compared to individuals and paired nonculture tests, culture was less than perfect.
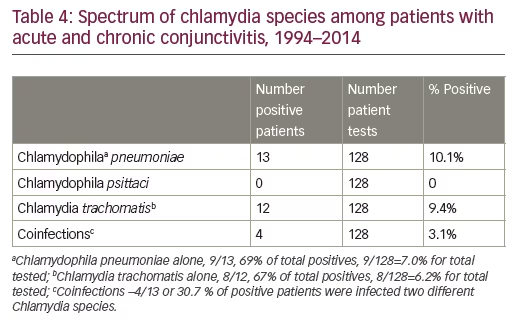
C. pneumoniae (n=13) was documented in 10.1% of the 128 screened samples versus 9.4 %, n=12 for C. trachomatis. Mixed chlamydia infections (C. trachomatis and C. pneumoniae) were found in four of the 13 (30.8%) positive samples or 3.1% of tested samples (see Table 4).
Discussion
We provide a historical and current snapshot of the prevalence of chlamydia in the South Florida. This is the largest series reported to date. C. trachomatis was documented for all age groups by multiple test methods. Similar to genital rates, neonates, adolescents, and young adults were identified as high risk groups. Interestingly in this population, rates were higher for males than for females for all test periods. Females are more likely to be screened and perhaps treated than males. Currently, males are not routine targeted for screening in the US.
We are also the first group to document the presence of C. pneumoniae in ocular tissues of patients presenting with acute and or chronic chlamydial disease outside of an endemic trachoma area. C. pneumoniae in our series were detected with greater frequency than C. trachomatis. Coinfections occur in at least three or more patients.
As in genital disease nucleic acid amplification tests (NAATs) were the most sensitivity laboratory method for detecting chlamydia in ocular disease for both evaluation periods. A variety of authors have also documented the validity of nucleic acid tests for documentation of chlamydia in ocular tissue. Hammerschlag and colleagues evaluated AMPLICOR for the detection of C. trachomatis in ocular and nasopharyngeal specimens from 75 infants with conjunctivitis. They found the sensitivity, specificity and positive and negative predictive values of PCR compared with culture to be equivocal at 92.3, 100, 100, and 98.4%, respectively.25
Kowlaski and colleagues have also documented the efficacy of molecular methods to detect and confirm the presence of C. trachomatis in ocular samples.26,27
Currently, there are no approved NAATs tests for ocular chlamydia testing in the US. DFA and cultures remain the gold standards and current CDC recommendations.22
Although there was a steep decline from baseline (13.4%, 1986–2004) to 6.0% for the most recent years (2010–2014), overall rate (6.0%) and rates for both males (7.6%) and females (4.6%) are equivocal or higher than the reported 1.7% for persons aged 14–39 years (NHANES, 2007–2012) and the 4.7% among sexually active females.
A total of 1,441,789 cases of genital chlamydia was reported in the US in 2014. The overall rate was 456.1 cases per 100,000 persons. Using the conservative rate of one case of ocular chlamydia for every 300 cases of genital disease, this would translate to 4,807 cases of ocular disease across the US or a rate of 1.52 per 100,000 persons. Miami-Dade is a highrisk area for chlamydia. The 2014 there was 10,814 reported cases for a rate of 406.1 per 100,000 people. The predicted rate for ocular chlamydia disease is 36 cases or a rate of 1.35 cases per 100,000. This rate is likely incorrect and is likely to be higher. We documented 32 cases among 532 patients during 2010–2014.
Our data indicate a high prevalence of chlamydia in a patient population in a high risk area of the US and could signal an increasing public health burden.
Limitations
This was a retrospective review with the intrinsic problems associated with such studies. Data from laboratory and chart review may have been incomplete. Over the 28 year period, methods and technology and the environment in which a laboratory test was performed could have impacted the performance of screening tests. Patients evaluated for ocular chlamydia in this study may not have been representative of the general population of the larger group of patients with ocular conjunctivitis.
There may have been selection bias among patients referred or directed to our institute due to economic or recalcitrant therapeutic problems. In addition, patient samples were requested and submitted by physicians with varying clinical expertise in recognizing chlamydia. At least half of the patients were pretreated and this may have affected the documentation of chlamydia in these patients.


